Invented by Russell G. Olsen, Marina V. Pascali, Merative US LP
Optimization of patient care teams involves the identification of the most effective team composition, which can vary depending on the patient’s needs. For instance, a patient with a chronic condition may require a team that includes a primary care physician, a specialist, a nurse, and a social worker. On the other hand, a patient who requires surgery may need a team that includes a surgeon, an anesthesiologist, and a nurse anesthetist.
The correlation between patient characteristics and care providers’ characteristics is essential in determining the most effective team composition. For instance, a patient with a chronic condition may require a care team that includes providers with experience in managing chronic conditions. Similarly, a patient who requires surgery may need a care team that includes providers with expertise in surgical procedures.
The market for optimization of patient care teams is growing, with healthcare organizations investing in tools and technologies that can help them identify the most effective team composition. These tools use data analytics and machine learning algorithms to analyze patient data and provider characteristics, identifying patterns and correlations that can inform team composition.
One example of such a tool is the Patient Care Team Optimization Platform developed by CipherHealth. The platform uses data analytics to identify the most effective team composition based on patient characteristics and provider expertise. The platform also provides real-time feedback to care teams, enabling them to make adjustments to their approach as needed.
The benefits of optimizing patient care teams are numerous. Patients receive better care, leading to improved outcomes and reduced costs. Providers also benefit from working in more effective teams, leading to increased job satisfaction and reduced burnout.
In conclusion, the market for optimization of patient care teams based on the correlation between patient characteristics and care providers’ characteristics is growing. Healthcare organizations are investing in tools and technologies that can help them identify the most effective team composition, leading to improved patient outcomes and reduced costs. As the healthcare industry continues to evolve, optimizing patient care teams will remain a crucial factor in achieving the goal of providing high-quality, cost-effective care.
The Merative US LP invention works as follows
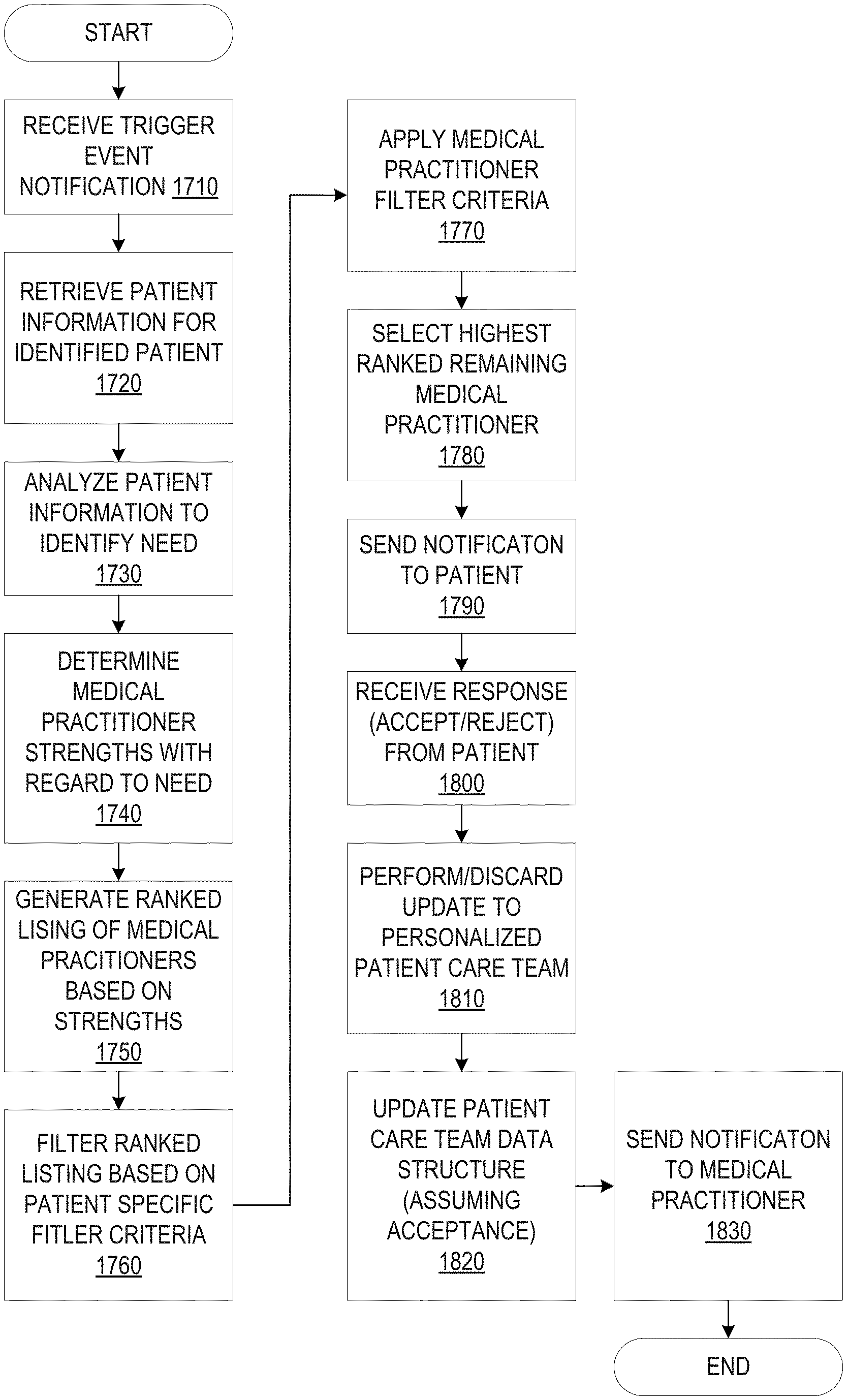
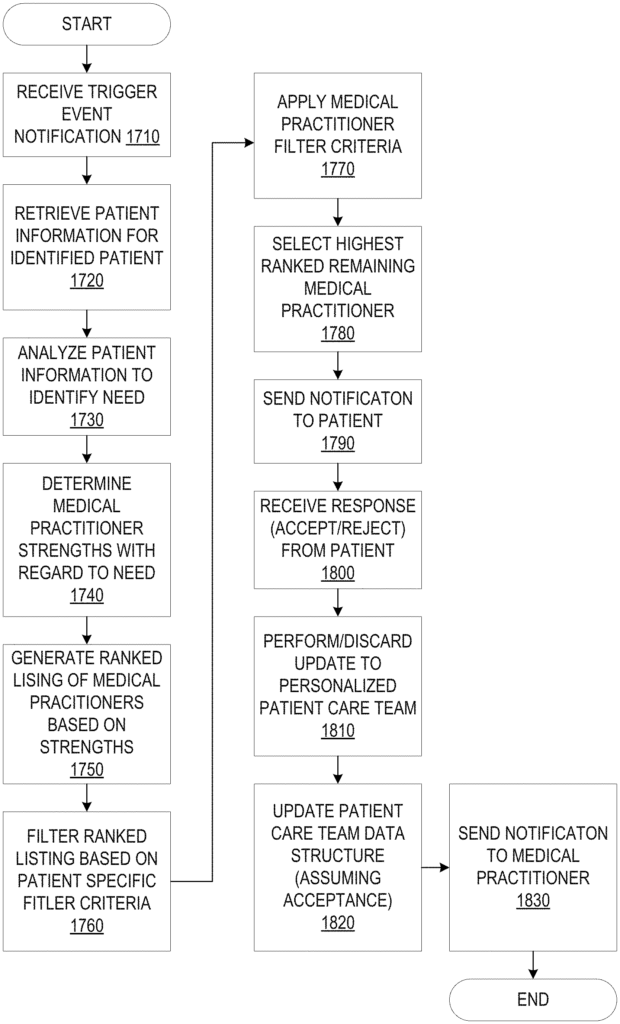
Mechanisms for matching patients with providers of care are provided.” The medical needs of a patient are determined by analyzing patient information from at least one source. Based on the results of the analysis, the patient information of a number of other patients who are associated with a group of care providers can be analyzed. For each of these care providers, the measure of strength is then determined for a particular type of medical treatment that corresponds to the one or more medical needs. The strengths of the care providers are used to select at least one provider for inclusion in the care team of the current patient. “A care team data structure containing information about at least one provider is output.
Background for Optimization for patient care teams based on correlation between patient characteristics and care providers characteristics
The present application is a general improvement in data processing and a method for determining the optimal patient care team by comparing patient characteristics with care provider characteristics.
Monitoring patients with chronic diseases, such as diabetes, congestive cardiac failure and asthma, is one of the biggest challenges in modern medicine. To manage chronic illness, patients need ongoing follow-up care and treatment. Unfortunately, many of these patients receive no treatment or care at all, only receive care on an sporadic schedule, or do not follow recommended guidelines. Even worse, many patients fail to perform the simple daily tasks that can prevent or reduce the severity and frequency of a catastrophe event like a hospitalization. These patients are often forced to suffer unnecessarily from the symptoms of chronic illnesses that could have been prevented or minimized with ongoing treatment and care. Some of these patients will need to be hospitalized or, in the most severe cases, may even die. This could have been avoided if they had received the right treatment and care.
This Summary is intended to present a number of concepts in a simplified format that are described in greater detail in the Detailed Description. This Summary does not aim to identify the key features or factors of the claimed matter. Nor is it meant to be used as a tool to limit the scope.
In one example, a method for matching care providers with patients is provided in a data-processing system that includes at least one processor. The method includes analyzing current patient information from at least a single patient information source, and determining at least one current medical need by the data processor system. The data processing system also analyzes patient information of a plurality other patients who are associated with a number of care providers. Based on the results of this analysis, the data processor determines a measure for strength of a type medical care that corresponds to the at-least one medical need for each of the care providers in the plurality. The method also includes selecting at least one provider of the plurality to be included in a team of care for the patient, based on strengths determined for each provider. The method also comprises generating, by the data-processing system, a data structure for a care team that includes information about at least one provider.
In other illustrative examples, a program that can be read by a computer is included in a computer-readable medium. When executed on a computer device, the computer readable software causes the device to perform different operations and combinations thereof, as described above in relation to the method illustrated embodiment.
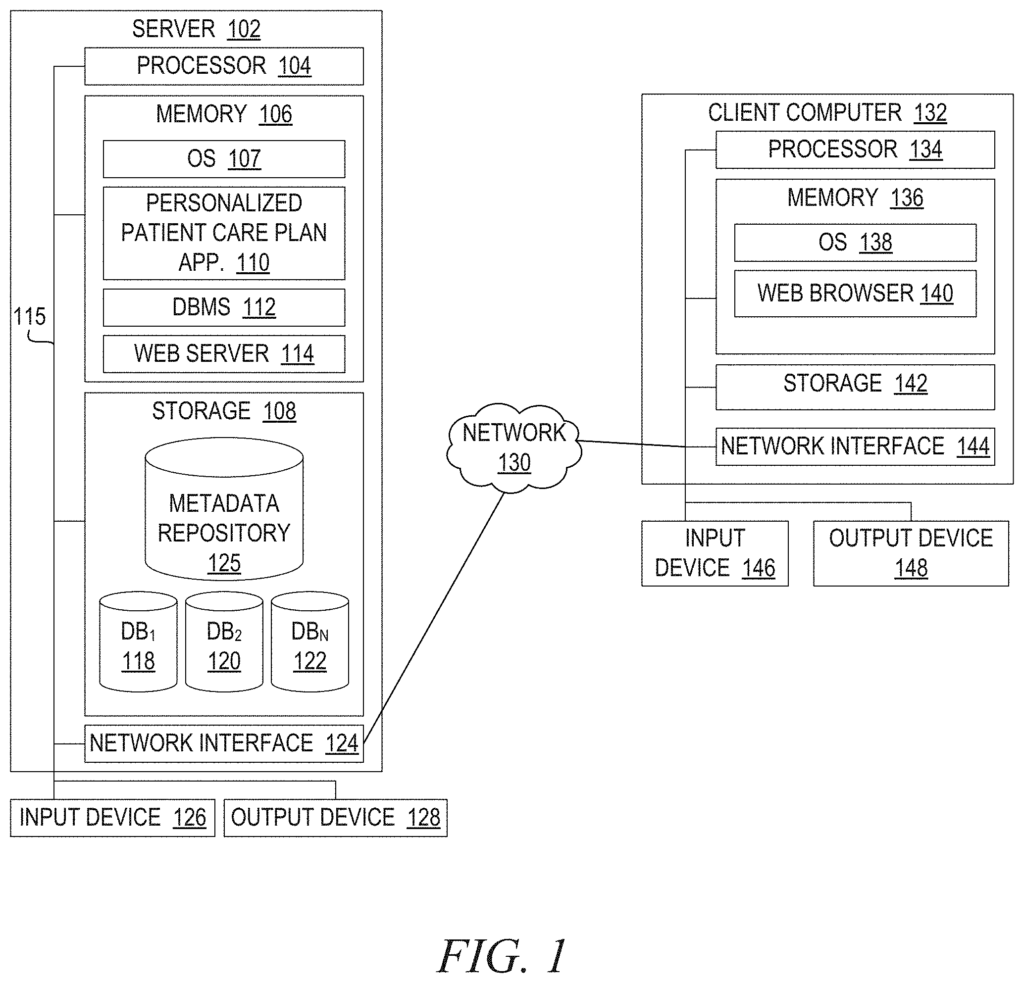
In yet another illustrative example, a system/apparatus may be provided. The system/apparatus can comprise one or multiple processors, and a memory coupled with the one or several processors. The memory can contain instructions that, when executed by one or more of the processors, cause them to perform a variety of operations and combinations thereof, as described above in relation to the method illustrated embodiment.
The following detailed description will show the features and benefits of the invention.
The term “mechanism” will be used throughout the description to refer to elements of the present invention that perform various operations, functions, and the like. The term “mechanism” will be used in this description to describe elements of the invention that perform different operations, functions and the like. A “mechanism” is a device. As used herein, the term “mechanism” can be an implementation of functions or aspects in the illustrative examples as an apparatus, procedure, or computer program product. In the case where a procedure is used, it can be implemented by a number of devices, apparatuses, computers, data-processing systems, etc. The logic represented by the computer code or instructions that are embodied on or in the computer program products is executed by hardware devices to perform the functions or operations associated with a specific “mechanism.” The mechanisms described in this document may be implemented by specialized hardware, general-purpose hardware running software, software instructions on a storage medium that are easily executable by general-purpose hardware or specialized hardware.
The present description and claims can use the terms “a”, “at least one”, and “one or more” In relation to specific features and elements in the illustrative examples. These terms and phrases should be understood to mean that at least one particular feature or component is present in an illustrative example, but more can be present. These terms/phrases do not limit or require a description or claim to only include a single element/feature. These terms/phrases do not require a minimum of one feature/element, but rather allow for a variety of features/elements to be included in the description or claims.
In the following description it is referred to as embodiments. It is important to understand that the invention does not limit itself to these specific embodiments. To implement and practice the present invention, it is possible to combine the following elements and features, regardless of whether they are related to different embodiments. The invention is not limited by the fact that embodiments may provide advantages over alternative solutions or over prior art. The following features, aspects, embodiments, and advantages are only illustrative, and not to be considered as elements or limitations in the appended claim(s), except when explicitly stated. The invention is also referred to in the text. “This document shall not be construed to be a generalization or limitation of any inventive subject matter disclosed in this document and shall not considered as an element or limit of the appended claim(s) except when explicitly stated.
In addition, the present description includes a plurality examples of different elements in the illustrative implementations. This is to illustrate further example implementations of illustrative manifestations and help with the understanding of their mechanisms. These examples are meant to be non-limiting, and they are not exhaustive in terms of the different possibilities of implementing the mechanisms for the illustrative exemplary embodiments. The present description will make it clear to those with ordinary skill that there are numerous alternative implementations of these elements which may be used in addition to or instead of the examples given herein, without departing the spirit and scope the present invention.
Overview
As noted above, the treatment and care of patients with illnesses that require ongoing treatment is an important issue in modern medicine. This ongoing treatment and caring is often a shared responsibility of the medical staff, such as doctors, nurses, etc. The patient is also responsible for the ongoing treatment and care. The patient and the medical worker.
A number mechanisms have been developed to assist the patient and medical worker in managing their shared responsibilities, including mechanisms to generate patient care plans based upon the patient’s condition, mechanisms to allow patients to monitor their own adherence to care plans, etc. These mechanisms tend to view patients as generic types, such as a generic type of asthmatic, generic diabetic, etc. It is possible to classify patients based on their age, gender and race. The care plan for the patient can be used by multiple patients with the same medical diagnosis and demographics. “The care plan is not personalized for the specific patient, but based on a general classification of the patient.
Each patient is unique because they have a different lifestyle. This uniqueness is not reflected by the care plans that are generated using known mechanisms.
That is to say, the patient care plan mechanisms that are known to us are designed to classify patients and assign them to generic categories. Then we apply generic care plans to those patients.” Although the mechanisms that employ such patient care plans mechanisms may refer them to as “personalized” While mechanisms employing such patient care plan mechanisms may refer to them as being?personalized? They may appear to be “customized” for the patient but in reality they are not. The patient is not presented with a plan of care that they feel is tailored to their needs. Patient care plans are not tailored to the individual patient, but can be used for a large number of patients with the same medical condition and demographics, such as all female 40-year-olds. “There are no mechanisms to personalize the treatment and care of a patient, based both on their medical condition and their own lifestyle. This includes taking into consideration multiple lifestyle conditions as well as the facilities and resources that the patient has available based upon their lifestyle.
It is important to understand that the word ‘lifestyle’ refers to a person?s way of living. As used in this article, the term ‘lifestyle’ refers to how a person leads their life. The term “lifestyle information” is used. The term ‘lifestyle information’ refers to data that is collected and characterizes a patient’s lifestyle. This may include various spatial, temporal, behavioral, environmental and other information. Lifestyle information is unique to a particular patient, and cannot be used to describe multiple patients. Depending on the implementation, lifestyle information can be presented at different levels of detail. This lifestyle information may include data generated by a specific patient using one or more computing devices, or other data communications devices, such as daily actions, schedules, preferences, etc. Lifestyle information could include, for example, the patient’s entry of information into a computer device running a patient tracker application, which indicates that the patient had breakfast in a fast-food restaurant at the airport this morning on his way to Virginia. The lifestyle information may also include data from external systems that are associated with third parties and characterize the patient?s lifestyle. For example, an insurance company might have information about a patient?s lifestyle (e.g. a smoker, overweight, inactive, at high risk of diabetes, etc.).
The temporal lifestyle data may include, for example, when the patient wakes up in the morning, when they eat, go to work and return home, take their children to school, shop for groceries, or go to bed at night, as well as other non-routine events, free time, scheduled flight, ferry, train, or other ground transportation departure/arrival times, or any other temporal information characteristic of the patient’s daily life or schedule. The temporal lifestyle data may include, for instance, the time the patient gets up in the morning, their meal times, their work schedules, their return to home from work, their time to take their kids to school, their grocery shopping, their bedtime, non-routine events that are scheduled, their free time, their scheduled flight times, their scheduled ferry or train departure/arrival time, as well as any other temporal details of their daily lives and non-routine planned events.
This information can include one or more data structures that identify locations associated with a patient’s everyday lifestyle, such as the location where they live, work, go to school, shop, visit their doctor, travel routes between these locations, etc. Spatial lifestyle information can also include information about the building’s number of floors or stories, such as a two-story house, five-story office, etc. and whether it has stairs. Geographic information such as the city, county, state or country where the patient resides, works, travels, or otherwise lives can be included in the spatial lifestyle information.
This information consists of one or more data structure with indicators of the environmental quality in environments where the patient is currently present, or is expected to be at a future time (based on temporal and spatial lifestyle), or is typically present every day or on a routine basis. Environmental lifestyle information can include, for example, information about a patient’s location at home, such as whether it is in a rural or urban environment, and whether they have access to walking trails, parks, etc. This environmental lifestyle data may include information on the patient’s workplace, such as whether they work in an office with fluorescent lighting and quiet or in a manufacturing environment with loud machinery and heavy noises. It could also be information about their office, including whether they use computers most of the time, have a private office, or are in a cubicle.
In relation to behavioral lifestyle information, these data structures contain indications of patient behavior and preferences, i.e. lifestyle preferences. The behavioral lifestyle information can include information such as the patient?s habits, their responses to different communication modalities, patterns and activities, etc. Such behavioral lifestyle information could indicate, for example, that the patient eats a snack each evening after 9 pm or walks his/her dogs in the mornings between 9 am and 5 pm. The behavioral lifestyle data may also indicate the patient’s preferences with respect to different elements of their daily lives, such as the types of food they like or dislike, the types of physical activities they enjoy/dislike, and when they like to do certain things, for example, exercising before/after work.
Click here to view the patent on Google Patents.
Leave a Reply