Invented by Pardis Sabeti, Andres Colubri, Todd Brown, Harvard College, Broad Institute Inc
Health data aggregation involves the collection and integration of various types of health-related data from multiple sources. This can include electronic health records, laboratory reports, patient-generated data, and even data from wearable devices. The aim is to create a comprehensive and holistic view of an individual’s health status or to monitor the health of a population. Aggregating this data allows for a more accurate assessment of disease prevalence, risk factors, and patterns, which is crucial for effective outbreak and epidemic modeling.
Outbreak modeling focuses on predicting and understanding the spread of infectious diseases within a defined population or geographical area. By analyzing data on disease transmission, population demographics, and environmental factors, outbreak models can estimate the likelihood and severity of an outbreak. This information is invaluable for public health officials and policymakers in planning and implementing appropriate interventions to control the spread of the disease.
Epidemic modeling takes outbreak modeling a step further by considering the dynamics of disease transmission on a larger scale. It aims to predict the course of an epidemic, including its peak, duration, and potential impact on healthcare systems. Epidemic models use complex mathematical algorithms and simulations to account for various factors such as population density, mobility, and social interactions. These models enable policymakers to make informed decisions about resource allocation, vaccination strategies, and other interventions to mitigate the impact of an epidemic.
The market for health data aggregation, outbreak modeling, and epidemic modeling is driven by several factors. Firstly, advancements in technology have made it easier to collect, store, and analyze large volumes of health data. The proliferation of electronic health records and the increasing adoption of wearable devices have provided a wealth of data that can be leveraged for modeling purposes. Additionally, the growing awareness of the importance of data-driven decision-making in public health has led to increased demand for these services.
Furthermore, the recent COVID-19 pandemic has highlighted the critical role of accurate modeling in managing outbreaks and epidemics. Governments and healthcare organizations worldwide have recognized the need for robust data analysis and modeling capabilities to guide their response efforts. This has further fueled the market growth, with investments pouring into research and development of innovative modeling techniques and software solutions.
The market for health data aggregation, outbreak modeling, and epidemic modeling is highly competitive, with numerous players offering a range of services and solutions. Established healthcare technology companies, research institutions, and startups are all vying for a share of this lucrative market. Key players in the market are continuously innovating to improve the accuracy and efficiency of their models, as well as to develop user-friendly interfaces and visualization tools.
In conclusion, the market for health data aggregation, outbreak modeling, and epidemic modeling is experiencing rapid growth due to the increasing demand for accurate and timely data analysis in public health. The advancements in technology, coupled with the lessons learned from recent outbreaks, have propelled this market forward. As the world becomes more interconnected, the need for effective modeling and prediction tools will only continue to grow, making this an exciting and promising field for both healthcare professionals and technology providers.
The Harvard College, Broad Institute Inc invention works as follows
The technology is based on aggregated health data, outbreak models and risk assessments to determine the likelihood of contracting COVID-19. The server of a healthcare organization provides COVID-19 kits and health apps to computing devices participating in the program. These applications log health data from users and record contacts with other participants via wireless interactions. The organization compares the data it receives with that received from other computing devices and identifies patterns. Based on the data, the server creates a model of an outbreak in a particular geographic area. The server sends the computing device of the user a calculated likelihood of the user contracting COVID-19. The server gives the outbreak model to users, healthcare workers or other people to use when responding to an outbreak.
Background for Health data aggregation, outbreak modeling and epidemic modelling
Public health policies focus on infectious disease surveillance, diagnosis methods and containment strategies. Users’ location histories and user contacts cannot be used to make user-specific diagnoses. The current technologies are not able to integrate information flows between user histories, healthcare professionals, vulnerable populations and third party actors who may be involved in quarantine and treatment, information dissemination and logistical activities. Healthcare providers, administrators, researchers in genomics, public health officials and quarantine and logistic personnel, as well as affected populations, perform independent assessments, following uncoordinated public health approaches. The technology available today only offers data collected from previous outbreaks, or computer extrapolations that are based on this limited data. Slow responses to an upcoming health concern could result in a greater risk for the public.
Citation of or identification of any documents in this application does not imply that the document was available prior to the invention.
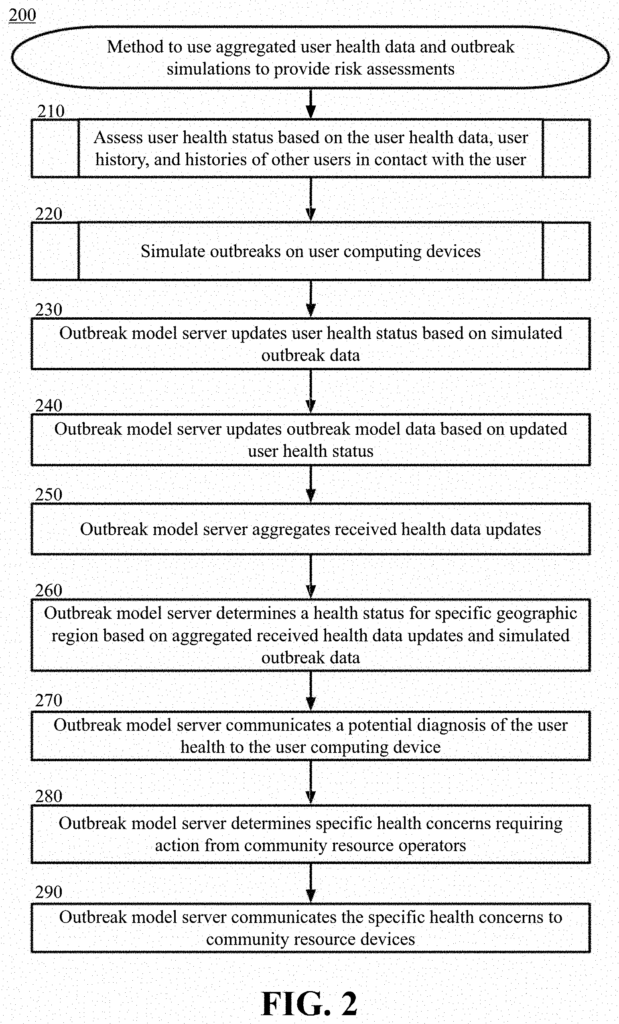
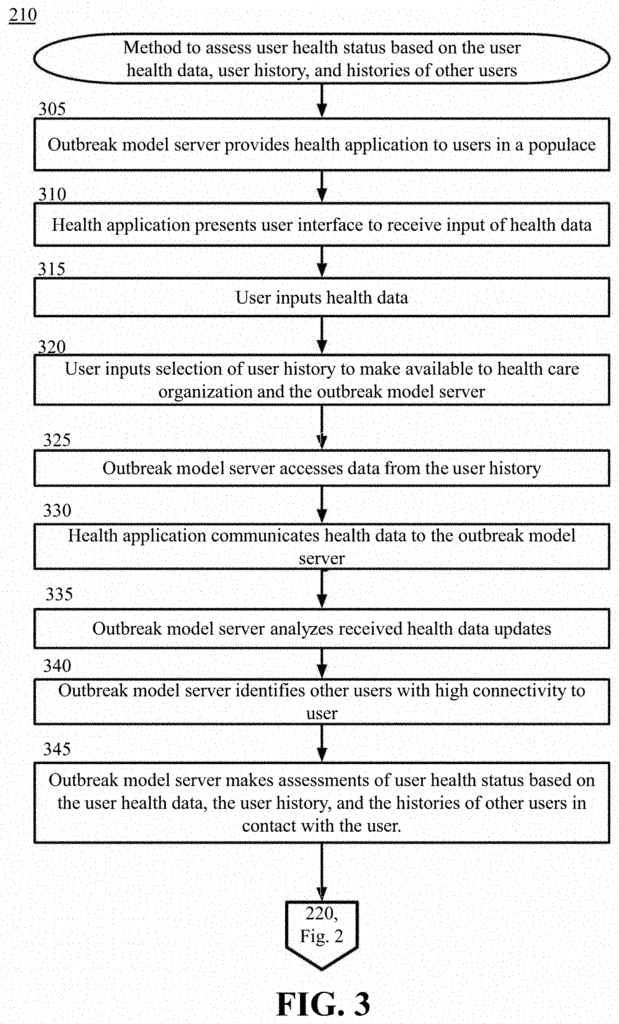
The technology described includes computer-implemented method, computer program product, and systems that use aggregated health data, outbreak models, to provide risk assessment. In some examples, the technology includes a server or device of a healthcare organization computing systems that receives a communication containing user health data and history data from a computing device associated with the user. The server, based in part on comparing the user’s health data with the health data of the other users and their user histories, identifies subsets of users who have a connectivity above a threshold. The server determines the common health data attribute from the user’s health data and health data of the subset of users, and then determines the health status of the individual based on at least part of the connectivity score and the common health data attribute. The server sends the health status to the computing device of the user for display.
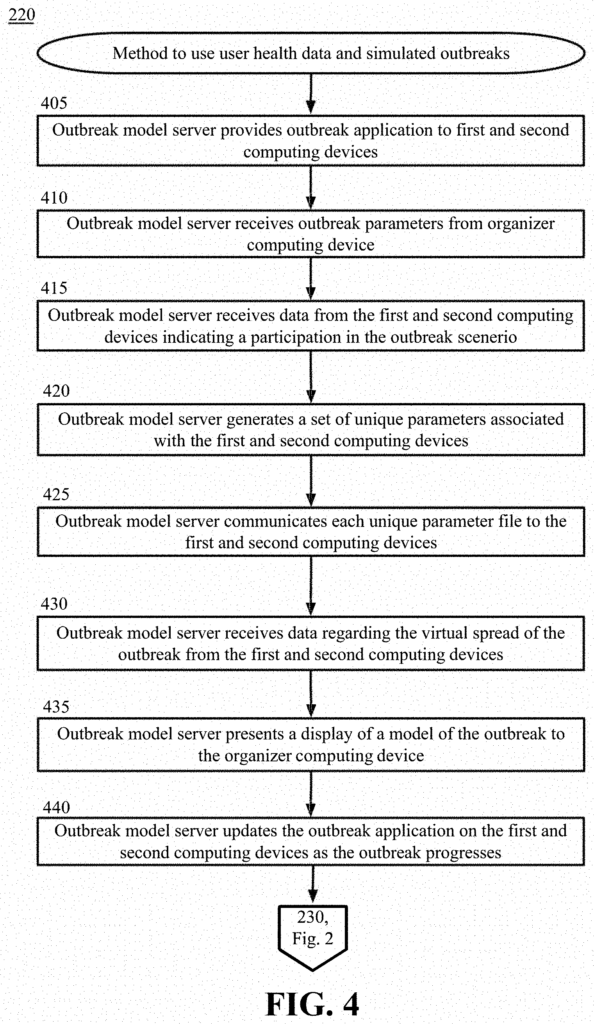
The server of the healthcare organization computing system receives from the outbreak organizer one or more parameters dictating characteristics for a simulated disease outbreak and notification that a specific user computing device participates in the simulation. The server creates a set user parameters for the specific user computing device that is participating in the disease simulation. This set of parameters is based, at least partially, on the parameters received and includes characteristics of the virtual user and the virtual pathogen. The server transmits a set of user parameter to the specific user computing device, and receives information about the spread of the virtual disease from the user computing devices. “The server displays a model of a simulated disease event using the data received.
The healthcare organization computing server integrates monitoring disease outbreak patterns and mechanisms into the overall healthcare data that is aggregated and shared by healthcare providers, researchers, and public health officials to support surveillance, detection and treatment activities more efficiently.
The following detailed description will reveal these and other features, aspects, and benefits of example embodiments to those with ordinary skill in this art.
Overview
In one aspect, the technologies described herein offer methods for automating health data extraction, diagnosis, and disease outbreak modelling. This would enable individual users, healthcare professionals, public health officials and genomic and computational research to share and interpret aggregate data more quickly and efficiently. This could reduce the time between surveillance, detection and treatment. The spatiotemporal modeling is crucial in all of these applications to better understand the risk factors of transmission. This allows us to adjust the size and timing of interventions to increase their chances of success. Predicting the epidemic risk for individuals to contract the illness over time and space can be used to identify subpopulations at increased risk, and inform interventions like quarantine. To control an epidemic effectively, it is important to be able to quickly identify those in a system who are at risk during an outbreak. In a pandemic situation, such models are difficult to develop due to the uncertainties in the pathogenic parameters and the urgency of the interventions.
In one aspect, the technology includes applications that users can use on their computing devices. The health application can be a downloadable app or an application programming interface that is used on a smartphone, or another user computing device to receive health data. Data may include demographics, contact information, location information, health data and other user-specific data. Health data can include symptoms such as a high temperature, coughing or congestion. Location data can include locations that the user visited recently using the computing device. Contact data can include people that the user comes in contact with at work, school, on social media, or any other way.
In another aspect, technology comprises applications and systems for modeling disease outbreaks. In some embodiments, outbreak modeling can be a simulated scenario. Applications may be provided for individual users that are capable of wireless communication and can record interactions with users within the simulation, as well as with other elements in the simulated environment. The application installed on the computing device of the user may use Bluetooth or another wireless protocol to send and receive “contact”. Other user computing devices running the health application, or other wireless devices within the simulation environment can be contacted. The initial parameters for the pathogen, and the initial conditions of the outbreak can be defined. The outbreak model is then based on the feedback received from individual interactions that are recorded and shared to a central or decentralized computing device. In other embodiments, individual interactions and initiation parameter may be based upon real-world conditions or interactions between individuals within a geographic area.
The two aspects are complementary, and can be combined. In another aspect, the technologies disclosed provide users with methods to integrate monitoring disease outbreak patterns and mechanisms into overall healthcare data that is shared between individual healthcare providers and researchers.
The term “disease” is used in the following ways: ?disease event,? ?outbreak,? ?epidemic,? ?pathogen,? Herein, the terms?pathogen’ and other similar terms are interchangeable to describe a scenario in which a disease or contagion is spreading throughout a population. The spread of disease is based on several factors, including the type of pathogens, contact between users and their locations, or the environmental conditions in which they are located.
The user could be asked to provide an affirmative response (i.e., enter a consent) before the data can be used. The user can restrict data usage, even if it is part of current technology or a third party use. The user can apply other restrictions on the use of data in order to protect their privacy and data.
Example Systems Architectures
Example embodiments are described in depth by turning to the drawings in which like numbers represent similar (but not necessarily identical), elements throughout the figures.
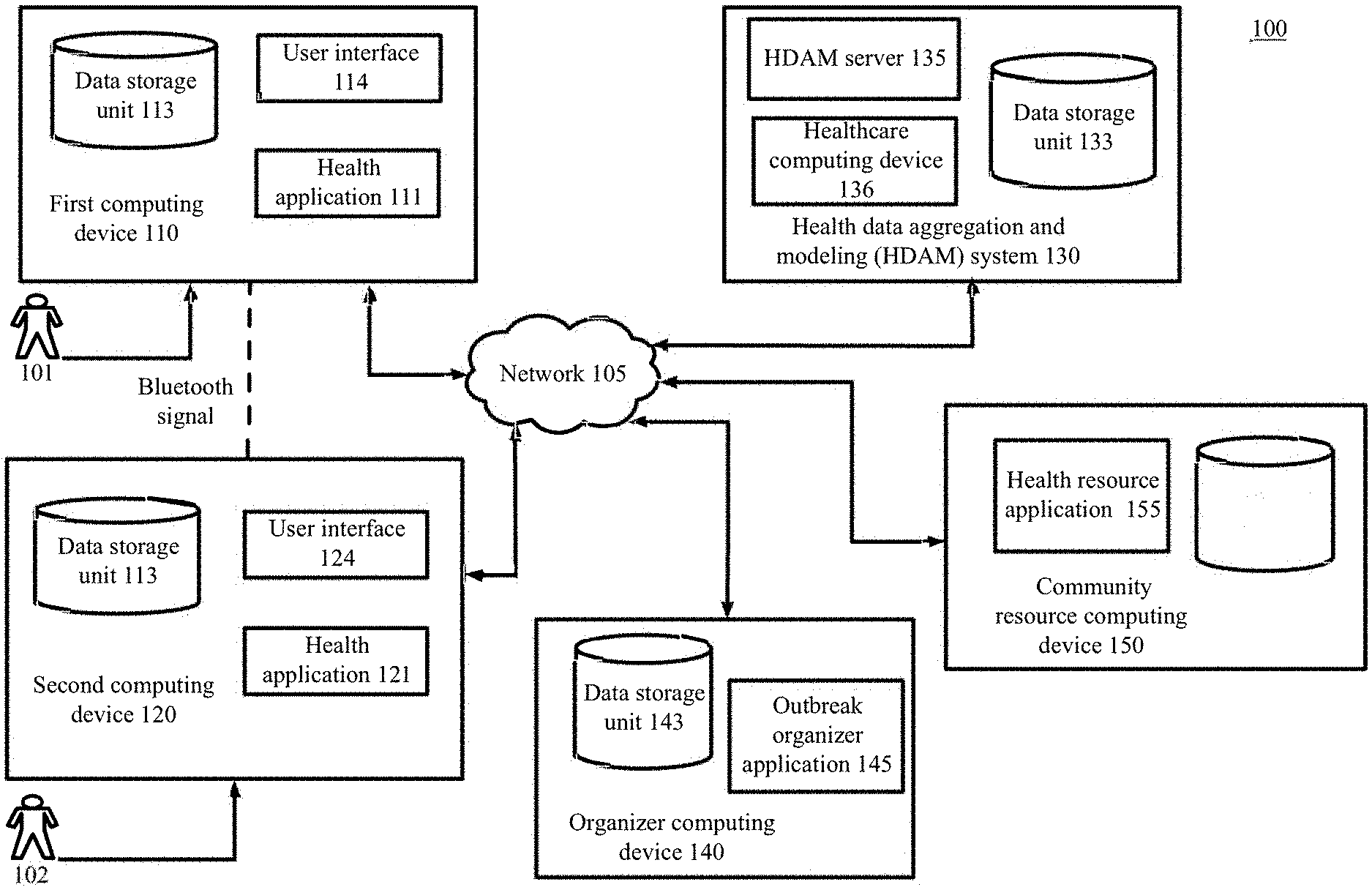
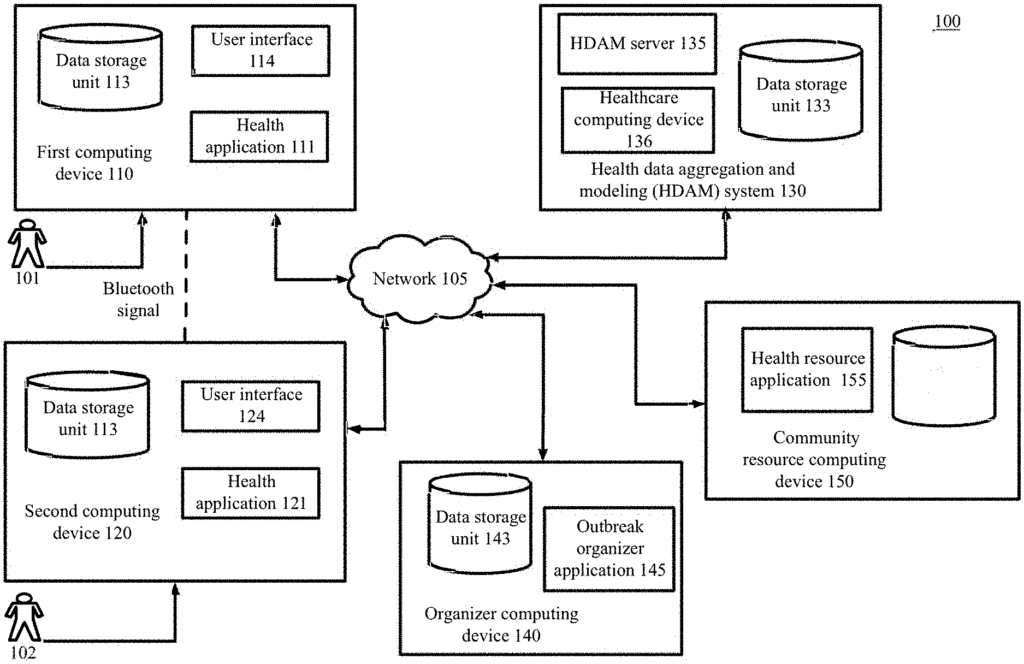
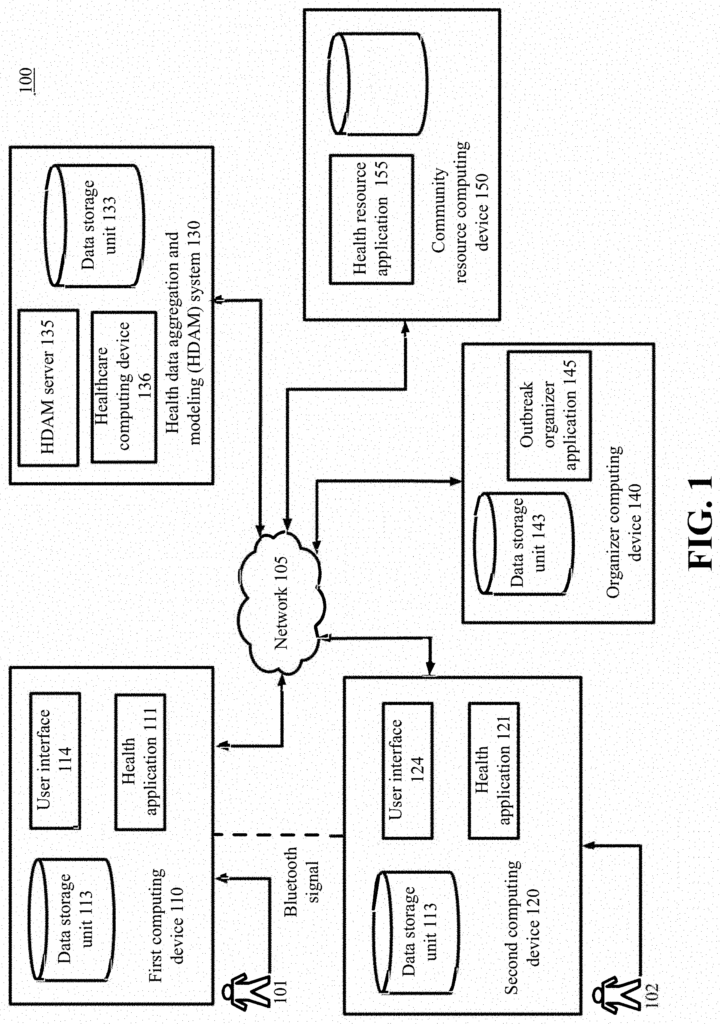
FIG. According to certain examples, FIG. 1 is a diagram showing a portion a simplified communication and processing architecture for a typical system that uses aggregated health data to perform outbreak modelling and provide risk assessments. In certain embodiments, the user associated with the user computing device 110, or 120, respectively, may be required to install an application such as the health application 111, or 121 and/or select a feature in order to benefit from the techniques described.
As shown in FIG. The system 100 includes a number of network computing devices, 110, 120. 130. 140. and 150, that can communicate via one or several networks 105, or any other suitable communication technology.
Each network includes a wired telecommunication system or wireless means that allows network devices (including those 110, 120 130 140 and 150) to exchange data. Each network 105 may include a local network (LAN) or a wide area network. Each network 105 can include a local area network (LAN? Storage area Network (?SAN? Personal area network (PAN) A metropolitan area network (MAN) Wireless local area network (WLAN) Virtual private network (VPN) Bluetooth, Near Field Communication (?NFC?) Ultra-wideband or any combination of these, or any other suitable architecture or system, that facilitates communication of data and signals. It should be understood throughout the discussion of the example embodiments that the term ‘data’ is used to refer to the data. The terms ‘data’ and ‘information? Herein, the terms?information? and ‘text’ are interchangeable to describe text, images or audio files, videos, or other forms of information in a computer environment. The communication technology used by devices 110,120,130,140,150 may be similar to network 105, or an alternative technology.
Each computing device of the network 110, 120 130 140 and 150 has a communication module that is capable of sending and receiving data via network 105. Each network device 110 can be a desktop computer, laptop, tablet, television, with embedded processors, or a TV coupled to it, or a smartphone, wearable or handheld computer or personal digital assistant. Wearable devices, such as smartwatches and glasses, can be used in conjunction with any processor-driven device. The example embodiment shown in FIG. “In the example embodiment shown in FIG.
The user can use the communication application on their user computing device 110 (which may be a standalone application or a web-browser application) to download, upload or access documents or web pages over a distributed network. The user computing device can communicate with other devices or web servers connected to the network, such as a webserver of the healthcare system 130. In another example the user computing device communicates with the devices in the Healthcare Organization System 130 using NFC, Bluetooth, WiFi, Infrared or any other suitable communication technology.
The user computing devices 110 use a wireless communication technology to communicate with other computing devices participating in the outbreak models, such as the second computing device 120. Wireless technology can be NFC, Bluetooth, WiFi, Infrared or another suitable wireless communication technology. Communication can take place even if different providers provided the user devices 110 and 120 or health applications 111 and 121. The healthcare organization 130, for example, may provide the health app 111 while a third party provided the app 121 on a second computing device. Because the two health apps 111,121 can recognize and communicate with different application types, the two devices 110,120 may still be able to perform the methods described here. “Any provider of health apps 111,121 can configure the applications to communicate between each other, the healthcare organization 130 or any other device or party.
Click here to view the patent on Google Patents.
Leave a Reply