Invented by Chien-Hsing Chang, David M. Goldenberg, Immunomedics Inc
The market for combination therapies in cancer treatment is constantly evolving, with researchers and pharmaceutical companies striving to find new ways to overcome resistance and improve patient outcomes. One promising combination that has shown great potential is the use of ABCG2 inhibitors in conjunction with Sacituzumab Govitecan (IMMU-132) to overcome resistance to SN-38 in Trop-2 expressing cancers.
Trop-2, also known as TACSTD2, is a cell surface glycoprotein that is overexpressed in various types of cancer, including breast, lung, colorectal, and pancreatic cancers. It plays a crucial role in tumor growth, invasion, and metastasis, making it an attractive target for cancer therapy. Sacituzumab Govitecan is an antibody-drug conjugate (ADC) that specifically targets Trop-2, delivering the potent cytotoxic drug SN-38 directly to cancer cells.
SN-38 is the active metabolite of irinotecan, a widely used chemotherapy drug. However, resistance to SN-38 can develop over time, limiting its effectiveness in treating cancer. This is where the combination with ABCG2 inhibitors comes into play. ABCG2, also known as breast cancer resistance protein (BCRP), is a drug efflux pump that actively transports SN-38 out of cancer cells, reducing its intracellular concentration and efficacy.
By combining ABCG2 inhibitors with Sacituzumab Govitecan, researchers aim to block the efflux of SN-38 from cancer cells, allowing for higher intracellular drug concentrations and overcoming resistance. Several ABCG2 inhibitors, such as Ko143, fumitremorgin C, and elacridar, have been studied in preclinical and clinical settings, showing promising results in combination with Sacituzumab Govitecan.
The market potential for this combination therapy is significant, given the prevalence of Trop-2 expressing cancers and the need for effective treatment options. Breast cancer, for example, is one of the most common cancers worldwide, and Trop-2 is overexpressed in approximately 90% of triple-negative breast cancers, a particularly aggressive subtype with limited treatment options. Lung, colorectal, and pancreatic cancers also represent significant markets for this combination therapy.
In addition to the potential market size, the combination of ABCG2 inhibitors with Sacituzumab Govitecan offers several advantages over traditional chemotherapy regimens. First, by specifically targeting Trop-2 expressing cancer cells, the therapy can potentially minimize off-target toxicities and improve patient tolerability. Second, the use of ADCs allows for targeted drug delivery, reducing systemic exposure and potential side effects. Finally, the combination therapy has the potential to overcome resistance to SN-38, improving patient outcomes and survival rates.
However, there are still challenges to overcome in bringing this combination therapy to the market. Clinical trials are ongoing to evaluate the safety and efficacy of ABCG2 inhibitors in combination with Sacituzumab Govitecan, and regulatory approval will be required before it can be widely used. Additionally, cost considerations and reimbursement policies will play a crucial role in determining the market adoption of this therapy.
In conclusion, the market for combination therapies involving ABCG2 inhibitors and Sacituzumab Govitecan to overcome resistance to SN-38 in Trop-2 expressing cancers holds great promise. With the prevalence of Trop-2 expressing cancers and the need for effective treatment options, this combination therapy has the potential to significantly improve patient outcomes. However, further research, clinical trials, and regulatory approvals are needed to fully realize the market potential of this innovative approach.
The Immunomedics Inc invention works as follows
The present invention is directed to therapeutic ADCs that comprise a drug coupled to an anticancer antibody or fragment of antigen-binding antibodies. The drug of choice is SN38. The antibody or fragment thereof is more preferably bound to Trop-2, and the therapy used to treat cancers that are Trop-2 positive. The antibody of choice is hRS7. ADC is given to a patient with cancer, in conjunction with ABCG2 inhibitor. Combination therapy is effective in treating cancers resistant to ADC or drug alone.
Background for Combination of ABCG2 Inhibitors with Sacituzumab Govitecan (IMMU-132) Overcomes Resistance to SN-38 for Trop-2 expressing Cancers
Resistance to chemotherapy by cancer cells has been a major problem for decades, and is responsible for approximately 90% of all cancer treatment failures” (Pluchino, et. al., Drug Resistance, Updates, 15: 98-105) Some cancers are intrinsically resistant to chemotherapeutics, while others develop drug resistance during treatment (Lippert, et. al. 2011, Int J Med Sci, 8: 245-253, Ricci, et. al. 2015, J Develop drugs 4:138). MDR is one of many ways cancer cells can develop resistance to chemotherapeutic drugs. This resistance is primarily caused by the efflux of active drugs catalyzed ATP binding cassette transporters (Ricci et. al., J Develop Drugs, 4:138). ABC transporters are a large family with many functions. However, only some of them appear to be involved in MDR. These include ABCB1, ABCC1 & ABCG2(Ricci, et. al., J Develop Drugs, 4:138). The ABCG2 is the most prevalent transporter in solid tumors. (Ricci, et. al., 2015. J Develop Drugs, 4:138).
While chemotherapy and systemic drug administration have been used widely in cancer treatment, the delivery of drugs via antibody-drug conjugates in recent years has increased the efficacy of anti-cancer agents. ADCs deliver conjugated drugs to cells that express disease-associated antibodies, such as tumor antigens. This reduces systemic exposure for normal tissues with lower expression levels of antigens or those that do not express them. The drug conjugate is usually released intracellularly following internalization of ADCs, but in some cases, extracellular release may occur from ADCs bound to cells. ABC transporters can cause tumors to develop resistance to anti-cancer agents, or to still show intrinsic activity. “Despite their success in treating cancers of all kinds, chemotherapeutics such as antibody-drug-conjugates (ADCs) lose their clinical activity with time. Examples include irinotecan, doxorubicin, paclitaxel, cisplatin, paclitaxel, cisplatin, cisplatin, cisplatin, cisplatin, cisplatin, cisptalina,
The occurrence of resistance to drugs in cancer cells is caused by a number of factors, including decreased uptake of soluble drug, activation of a drug-detoxifying system, modulation or mutations of drug targets and defective apoptosis pathway. According to Vasiliou et. al. (2009, Hum Genom 3:128-90), the human genome contains 49 ABC genes, which are classified into seven subfamilies based on their sequence homology and order of the transmembrane domain (TM) and nucleotide binding folds (NBFs). ABCB1 (also called MDR1 or Pgp), ABCC1(also called MRP1) and ABCG2(also known BCRP, MXR or ABC-P) are the three ABC subfamilies that have been studied most extensively.
Members of the ABC superfamily can be expressed as either a half- or full-transporter. Full-transporters typically contain two nucleotide binding folds (NBFs) and two transmembrane domains. The TM domains are involved in substrate recognition and translocation, and the cytosolic ATP-bound NBFs drive transport. A half-transporter, on the other hand, has just one TM and one NBF and must be homodimers, or heterodimers, to function. ABCB1 is a notable full-transporter, whose substrates are vinca alkaloids (synthetic and natural), anthracyclines (natural or synthetic), epipodophyllotoxins (chemicals), taxanes (chemicals), irinotecan(chemical) and SN38(chemical). “The five members of the ABCG family are half-transporters” (Vasiliou et. al. 2009, Hum Gen 3:281-9). ABCG2 is known to mediate cellular resistance to SN38 (Brangi et. al. 1999, Cancer Res 59 :5938-46, Kawabata et. al. 2001, Biochem Biophys Res Commun 280 :1216-23) as well as tyrosine kina
Multiple approaches have been developed to overcome MDR. PSC-833, a second generation ABCB1 modifier (Twentyman & Bleehan 1991, Eur. J. Cancer. 27:1639-42) restored the sensitivity to inotuzumab-ozogamicin in ABCB1 expressing sublines in Daudi and Raji Lymphoma. This was due to the hydrophilic linker used to conjugate DM1 with antibodies (Kovton et. al., 2010 Cancer Res 70:2528-2537). It is also possible that the ABCB1 expressing cells are better able to retain a cytotoxic metabolite produced by this method. In addition, Ramsay and Dilda (2014), Front Pharmacol 5, 181 found that targeting detoxifying enzymes such as glutathione-S-transferase with intracellularly active prodrugs showed promise. The rationale for using ABC transporter inhibitors to overcome MDR was not successful in clinical trials. This could be due to the imperfection of the inhibitors or inadequate study design. The problem is being addressed through the development of newer agents that have greater substrate specificity and potency. They also have lower toxicity and better pharmacokinetics.
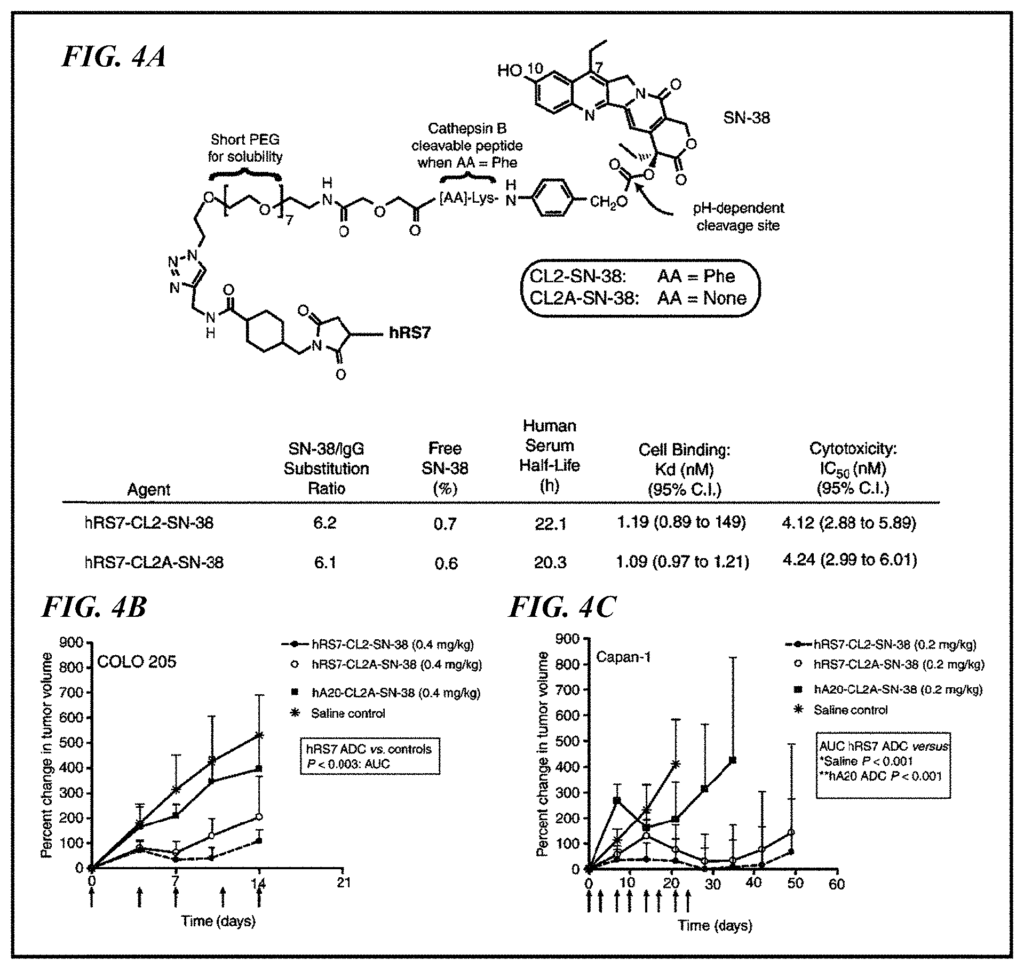
Sacituzumab Govitecan” (also known as IMMU-132) is a Trop-2-targeting ADC derived from SN-38, an active metabolite derived from irinotecan. IMMU 132 differs from other ADCs by using a drug that is not ultra-toxic, a high drug-to-antibody ratio (DAR), and a linker with a pH-sensitive cleavable to cause cytotoxicity in both the tumor and surrounding cells (Cardillo et. al. 2011, Clin Cancer Res 17, 3157-69, Cardillo et. al. 2015, Bioconjugate Chemistry 26:919-931, Goldenberg This novel ADC has been tested in clinical trials on patients with triple-negative advanced breast cancer (Starodub and al. 2015, Clin Cancer Res 21, 3870-8), urothelial cancer (Faltas and al. 2016, Clin Genitourinary Cancer 14, e75-9), as well as other solid tumors. The expression of MDR gene is likely to be present in these patients, as they have all received heavy chemotherapy. This may impact the therapeutic outcome for IMMU-132. “There is a need for improved ways to use ADCs such as IMMU-132 to treat cancers resistant to chemotherapy.
The present invention addresses an unmet need in the field by providing improved compositions and methods for treating drug resistant tumors using a combination anti-Trop-2 ADC with an ABC transporter inhibitor, preferably ABCG2. The ADC is more preferably conjugated with SN-38. A person with ordinary skill would realize that other drugs could be included in the ADC. The disclosed compositions and methods are useful for treating a wide range of diseases that are resistant to or less responsive than other therapies. The combination therapy can be used to treat a variety of diseases and conditions, including cancers that are positive for Trop-2, such as pancreatic metastatic cancer, triple negative breast cancer, urothelial carcinoma, small cell lung or non-small lung cancer.
Preferably the ADC incorporates a bispecific or multivalent anti-Trop-2, antibody fragment or any other antibody-based compound or molecule. The antibody can have different isotypes. Preferably, it will be human IgG1, IgG2, IgG3, or IgG4. More preferably, the hinge and constant regions of human IgG1 are included. The antibody can be humanized, humanized with murine hypervariable regions (CDR), humanized human-primate or fully human. ), as described by van der Neut Kolfschoten et al. (Science 2007; 317:1554-1557). The antibody or fragment thereof can be selected or designed to contain human constant region sequences belonging to specific allotypes. This may reduce immunogenicity in the ADC when administered to human subjects. Allotypes that are preferred for administration include non-G1m1 (nG1m1) allotypes, such as G1m3, G1m3,1, G1m3,2, or G1m3,1,2. The allotype should be selected from the group of nG1m1, nG1m1,2, and Km3 allotypes.
In There There T The
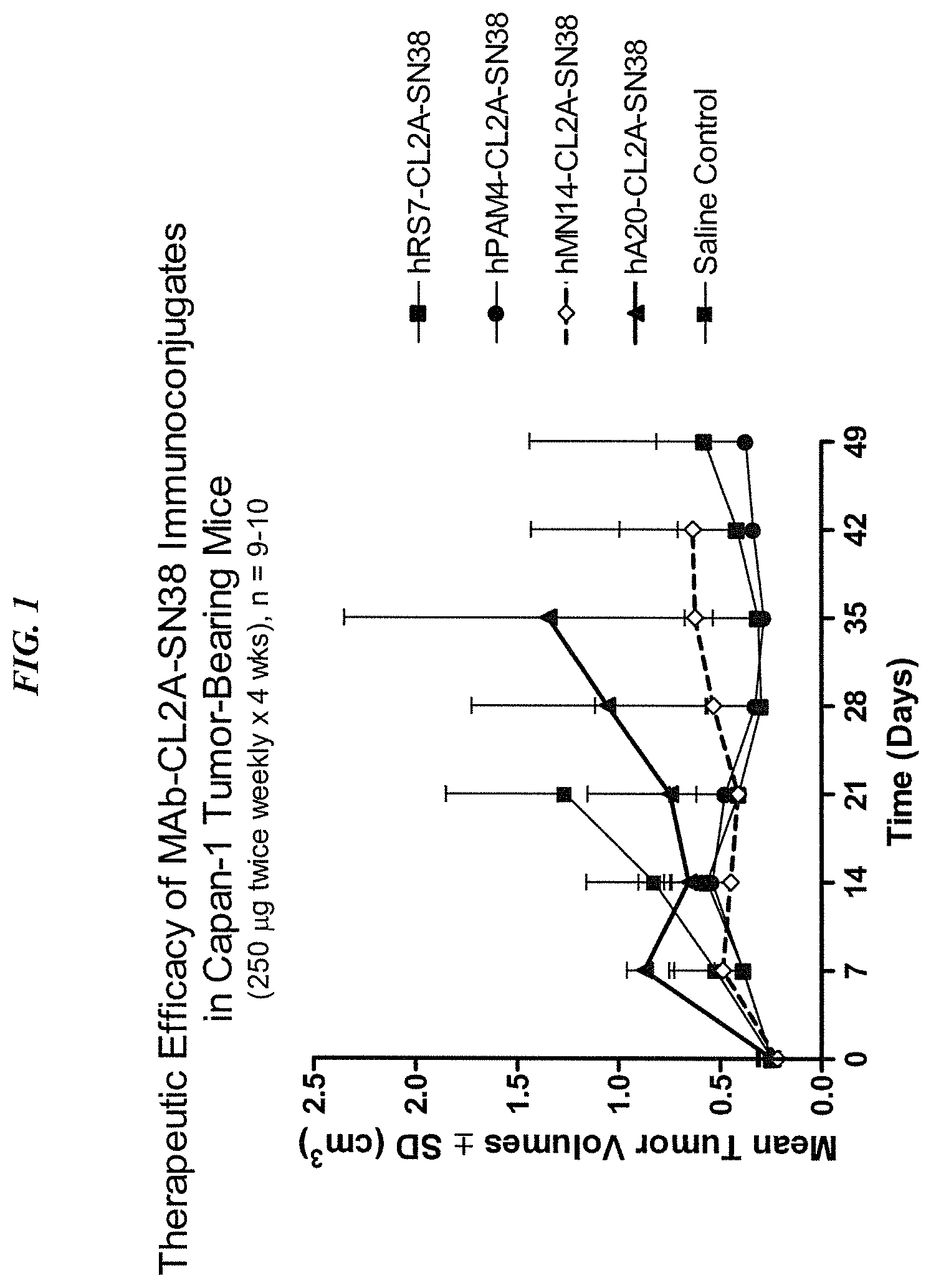
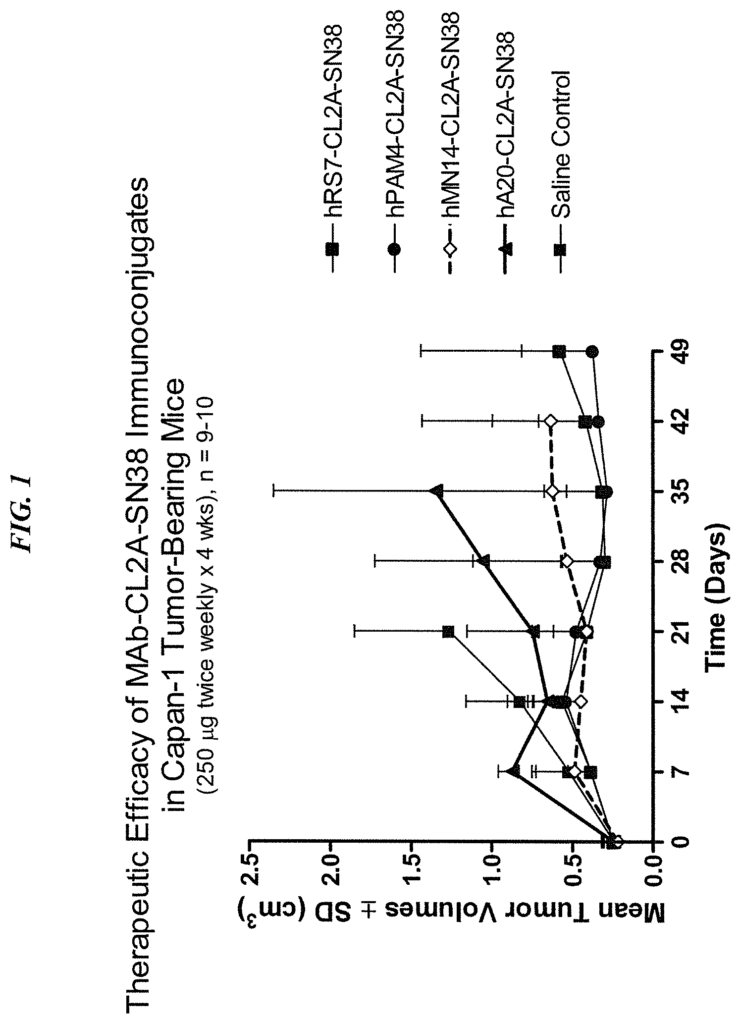
Exemplary antibody that can be used include but are not restricted to hR1(anti-IGF-1R) (U.S. Patent Application Ser. No. No. 12/722 645, filed March 12, 2010), hPAM4 (anti-mucin, U.S. Pat. 12, 2010), hPAM4 (anti-mucin, U.S. Pat. No. 7,282,567), hA20 (anti-CD20, U.S. Pat. No. 7,251,164), hA19 (anti-CD19, U.S. Pat. No. 7,109,304), hIMMU31 (anti-AFP, U.S. Pat. No. 7,300,655), hLL1 (anti-CD74, U.S. Pat. No. 7,312,318), hLL2 (anti-CD22, U.S. Pat. No. 7,074,403), hMu-9 (anti-CSAp, U.S. Pat. No. 7,387,773), hL243 (anti-HLA-DR, U.S. Pat. No. 7,612,180), hMN-14 (anti-CEACAM5, U.S. Pat. No. 6,676,924), hMN-15 (anti-CEACAM6, U.S. Pat. No. 7,541,440), hRS7 (anti-EGP-1, U.S. Pat. No. 7,238,785), hMN-3 (anti-CEACAM6, U.S. Pat. No. No. The antibody may be IMMU31 (anti AFP), hRS7, hL243, IMMU114, hL243g4P, hL243gamma4P, hA20, hA19, hLL1 or hLL2 as well as hA19, hA20, hA20 or hA20. The terms epratuzumab, hLL2, veltuzumab, hL243g4P (hL243gamma4P), and IMMU114 are interchangeable in the present application.
Alternative antibodies of use include, but are not limited to, abciximab (anti-glycoprotein IIb/IIIa), alemtuzumab (anti-CD52), bevacizumab (anti-VEGF), cetuximab (anti-EGFR), gemtuzumab (anti-CD33), ibritumomab (anti-CD20), panitumumab (anti-EGFR), rituximab (anti-CD20), tositumomab (anti-CD20), trastuzumab (anti-ErbB2), lambrolizumab (anti-PD-1 receptor), nivolumab (anti-PD-1 receptor), ipilimumab (anti-CTLA-4), abagovomab (anti-CA-125), adecatumumab (anti-EpCAM), atlizumab (anti-IL-6 receptor), benralizumab (anti-CD125), obinutuzumab (GA101, anti-CD20), CC49 (anti-TAG-72), AB-PGI-XG1-026 (anti-PSMA, U.S. patent application Ser. No. 11/983,372, deposited as ATCC PTA-4405 and PTA-4406), D2/B (anti-PSMA, WO 2009/130575), tocilizumab (anti-IL-6 receptor), basiliximab (anti-CD25), daclizumab (anti-CD25), efalizumab (anti-CD11a), GA101 (anti-CD20; Glycart Roche), muromonab-CD3 (anti-CD3 receptor), natalizumab (anti-a4 integrin), omalizumab (anti-IgE); anti-TNF-? “antibodies such as CDP571 by Ofei et. al. (2011) Diabetes 45:881-885, MTNFAI (Thermo, Rockford, Ill.), M302B and M303 from Thermo, Abbott Park, Ill.,
The chemotherapeutic moieties that may be used include taxanes (e.g., baccatin III, taxol), epothilones, anthracyclines (e.g. doxorubicin (DOX), epirubicin morpholinodoxorubicin cyanomorpholino-doxorubicin cyanomorpholino-doxorubicin cyanomorpholino-doxorubicin (2PDO However, other chemotherapeutic moieties that may be utilized include taxanes (e.g, baccatin III, taxol), epothilones, anthracyclines (e.g., doxorubicin (DOX), epirubicin, morpholinodoxorubicin (morpholino-DOX), cyanomorpholino-doxorubicin (cyanomorpholino-DOX), 2-pyrrolinodoxorubicin (2-PDOX) or a prodrug form of 2-PDOX (pro-2-PDOX); see, e.g., Priebe W (ed. ACS Symposium Series 574, Washington D.C. 1995, 332pp. Nagy et.al., Proceedings of the National Academy of Sciences, p. Natl. Acad. Sci. Sci. New Drugs, 17:361-373 (1998)) and similar compounds. The antibody or fragment thereof should link to at least one moiety of a chemotherapeutic drug; more preferable, 6 or more moieties. Most preferred, 6 to 8 moieties.
The cancers that may be treated by the methods and compositions include, but are not limited to, non-Hodgkin lymphomas; B-cell acute or chronic lymphoid lymphomas; Burkitt lymphoma; Hodgkin lymphoma; acute large B cell lymphoma and hairy-cell leukemias. These carcinomas can include those of the esophagus and gastrointestinal tracts, lungs, colons, breasts, uterus endometriums, cervixs, bladders, urotheliums, pancreas bone, brain connective tissue, liver gall bladder urinary bladder kidney skin, central nervous systems, testes. The cancer must express the Trop-2 antigen.
In certain embodiments of cancer treatment, anti-Trop-2 ADC therapy and ABCG2 inhibition may be combined with standard anticancer treatments such as surgery and radiation therapy. Combination therapies allow for lower doses to be administered of each therapy, reducing side effects and possibly reducing the number of courses of treatment required. “When there is minimal or no overlap in toxicity, full doses of both can be given.
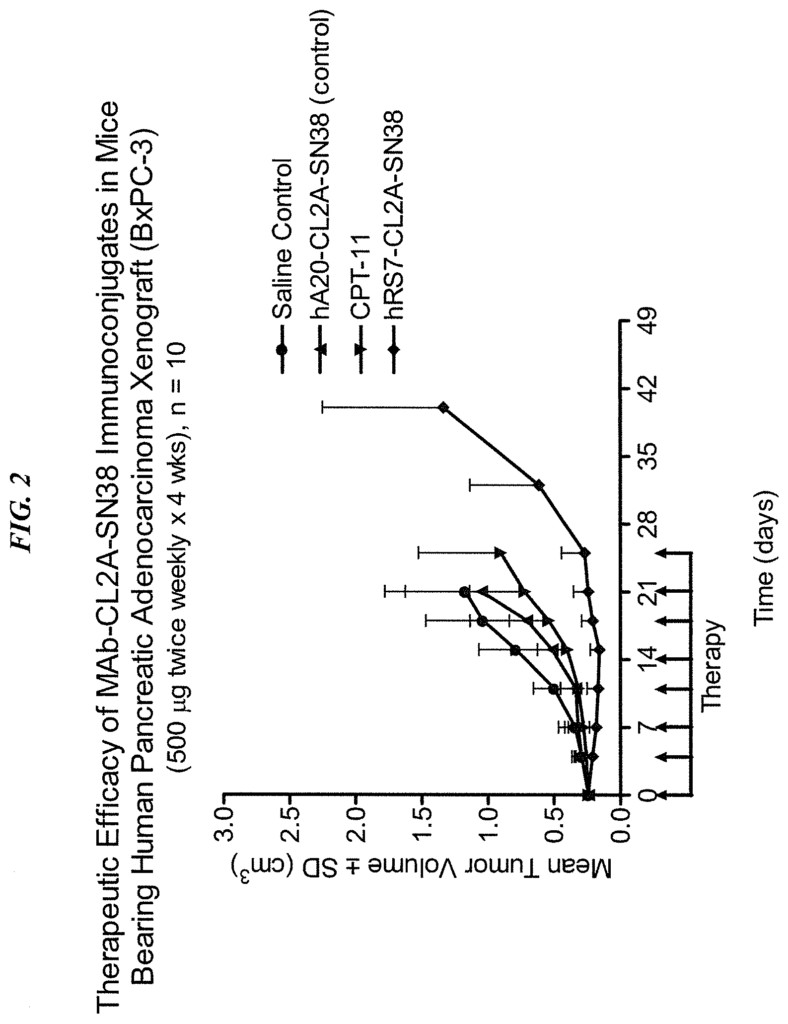
The optimal schedule of ADC can include two consecutive weeks of therapy followed by one, two, three or four weeks of rest, or alternate weeks of therapy and rest. The optimal schedule of dosing may include two consecutive weeks’ therapy, followed by alternating weeks between therapy and rest. It could also include a week of treatment followed by alternating weeks with rest. The treatment can be extended to any number of cycles. Preferably, at least 2, but preferably at minimum 4, 6, 8, 10, 12, 14, 16, or more. The dosage can be as high as 24 mg/kg. Examples of dosages include: 1 mg/kg; 2 mg/kg; 3 mg/kg; 4 mg/kg; 5 mg/kg 6 mg/kg 7 mg/kg 8 mg/kg 9 mg/kg 10 mg/kg 11 mg/kg 12 mg/kg 13 mg/kg 14 mg/kg 15 mg/kg 16 mg/kg 17 mg/kg 18 mg/kg. The preferred dosages are 4, 8, 9, 10 or 12 mg/kg. A person with ordinary skill would realize that many factors such as age and general health as well as specific organ function and weight as well as the effects of previous therapy on specific organs (e.g. bone marrow), may be taken into consideration when selecting the optimal dosage of ADC. The dosage and/or the frequency of administration can be changed during therapy. The dosage can be repeated as necessary, and tumor shrinkage is evident after only 4 to 8 doses. The optimized doses and schedules disclosed herein have shown unexpectedly superior efficacy with reduced toxicity on human subjects. The superior efficacy allows the treatment of tumors previously resistant to standard anti-cancer treatments, including CPT-11 (irinotecan), which SN-38 was derived from in vivo.
The methods described may include the use of CT, PET/CT or MRI to monitor tumor response. The blood levels of tumor markers such as CEA, CA19-9 (carcinoembryonic anagen), AFP, CA15.3, or PSA may be monitored. The dose and/or schedule of administration may need to be adjusted based on the results from imaging or marker blood levels.
The unexpected tolerability with the compositions and methods claimed in the instant patent is that even high doses of the antibody-drug conjugate can be tolerated, resulting only in low-grade toxicities such as nausea and vomiting or manageable neutropenia. Another surprising result is that the antibody-drug combination does not accumulate, unlike products which have conjugated SN38 to PEG, albumin or other carriers. This lack of accumulation correlates with better tolerability, and a lack of serious toxicities even after repeated doses or higher dosages. These unexpected results allow for optimization of the dosage and delivery schedule with high efficacies but low toxicities. The claimed methods allow for solid tumors to shrink by 15% or more (measured by the longest diameter) in patients with previously resistant cancers. A person with ordinary skill would realize that the size of a tumor can be measured in a number of ways, including total tumor volume, maximum tumor size in any one dimension, or a combination. This can be done with standard radiological techniques, such as computed-tomography, ultrasound, or positron emission tomography. It is not important how you measure the size, but rather that there is a tendency for tumors to shrink with ADC or ABCG2 inhibitor therapy. This should ideally result in complete elimination of tumors.
In particular preferred embodiments, ADCs and dosing regimens can be effective in patients who are resistant to standard treatments. ADC anti-Trop-2 hRS7 SN-38, combined with ABCG2 inhibition, can be given to a patient that has failed to respond to previous therapy with irinotecan (the parent agent of SN-38) Unexpectedly, irinotecan resistant patients may respond to hRS7 SN-38 in combination with ABCG2 inhibitor. ADCs that target tumor tissue specifically may improve targeting and enhance delivery of the therapeutic agents, while a combination of ADCs and ABCG2 inhibitors may be effective for tumors with active mechanisms to eliminate SN-38. Other antibody-SN-38 ADCs, such as IMMU-130 (anti-CEACAM-5-SN-38) or IMMU-140 (anti-HLA-DR-SN-38) may show similar improved efficacy and/or decreased toxicity when used with an ABCG2 inhibitor, compared to alternative standard therapeutic treatments. The preferred subjects may include a patient with metastatic colorectal or pancreatic cancer, as well as a patient with triple-negative breast carcinoma, who is HER+ and ER+ while also being progesterone-positive, and a patient with metastatic non-small cell lung cancer.
Definitions
The following terms will be used in the description to help you understand the subject matter. The terms that are not defined explicitly herein will be used according to their ordinary and plain meaning.
Click here to view the patent on Google Patents.
Leave a Reply