Invented by Zhu Chen, Kenneth P. Ellsworth, James A. Milligan, Elizabeth Oldham, Dietmar Seiffert, Vaishnavi Ganti, Mohammad Tabrizifard, Bianka Prinz, Merck Sharp and Dohme LLC, Adimab LLC
Cardiovascular diseases, including heart attacks and strokes, are the leading cause of death globally. According to the World Health Organization, an estimated 17.9 million people die each year due to cardiovascular diseases, accounting for 31% of all global deaths. This alarming statistic has led to a surge in research and development efforts to find innovative therapies to prevent and treat these conditions.
Factor XI is a protein that plays a crucial role in the blood clotting process. However, excessive activation of factor XI can lead to the formation of blood clots, which can block blood vessels and cause severe complications. Anti-coagulation factor XI antibodies work by inhibiting the activity of factor XI, thereby reducing the risk of blood clot formation.
The market for anti-coagulation factor XI antibodies is driven by several factors. Firstly, the increasing prevalence of cardiovascular diseases has created a significant need for effective treatment options. Traditional anticoagulant drugs, such as warfarin and heparin, have limitations and can cause adverse side effects. Anti-coagulation factor XI antibodies offer a more targeted approach with potentially fewer side effects.
Secondly, advancements in biotechnology and antibody engineering have facilitated the development of highly specific and potent anti-coagulation factor XI antibodies. These antibodies can selectively bind to factor XI and inhibit its activity, providing a more precise and efficient therapeutic approach.
Furthermore, clinical trials have demonstrated promising results for anti-coagulation factor XI antibodies. For example, a recent phase II trial conducted by a leading pharmaceutical company showed that an anti-coagulation factor XI antibody significantly reduced the risk of venous thromboembolism without increasing the risk of bleeding. These positive outcomes have generated enthusiasm among healthcare professionals and investors, further driving the market growth.
However, challenges remain in the market for anti-coagulation factor XI antibodies. The high cost of development and production of biologic drugs can limit their accessibility and affordability, particularly in developing countries. Additionally, regulatory approval processes can be time-consuming and costly, further delaying the availability of these therapies to patients.
Despite these challenges, the market for anti-coagulation factor XI antibodies is expected to witness substantial growth in the coming years. The increasing demand for effective and safe treatment options for cardiovascular diseases, coupled with advancements in antibody engineering and positive clinical trial results, will drive the market expansion. Moreover, ongoing research and development efforts aim to improve the efficacy and safety profiles of these antibodies, further boosting their market potential.
In conclusion, the market for anti-coagulation factor XI antibodies is experiencing significant growth due to the rising prevalence of cardiovascular diseases and the increasing demand for effective treatment options. These antibodies offer a targeted and potentially safer approach to preventing blood clot formation. While challenges exist, the market is expected to expand as research and development efforts continue to enhance the efficacy and accessibility of these therapies.
The Merck Sharp and Dohme LLC, Adimab LLC invention works as follows
The anti-FXI antibodies that bind to the apple 2 domain and inhibit activation by coagulation factors XIIa have been described.
Background for Anti-coagulation factor XI antibodies
(1) Field of the Invention.
The present invention is a set of antibodies that bind to the apple 2 domain in human coagulation factors XI and inhibit activation by coagulation factors XIIa.
(2) Description of Related Art.
Thromboembolic diseases, including both arterial and venous thrombosis remain the leading cause for morbidity and death in the Western World despite the availability and use of many anticoagulants such as heparins and vitamin K antagonists. (Weitz, et. al., Chest, 2008, 133, 234S-256S; Hawkins Pharmacotherapy, 2004, 24:62S-665S). They are effective at reducing the risk of thrombosis, but have multiple limitations. VKAs, for example (e.g. Warfarin has been the mainstay of oral anticoagulation, but the management of VKA treatment is complex due to the significant bleeding risks, the slow onset of action and the offset of its effect, as well as the multiple drug and dietary interactions (Hawkins op. cit. ; Ansell J et al., Chest 2008, 133:160S-198S). These new anticoagulants, which include rivaroxaban and apixaban as well as edoxaban and dabigatran, have shown at least non-inferior effectiveness compared to warfarin. They also require less monitoring and there are fewer food and drug interactions. The NOACs do increase bleeding risk as shown by the 18% annual incidence rate of major or minor clinically significant bleeding that was observed in the registration trials of the NOACs for stroke prevention of atrial fibrillation. (Connolly, et. al. N Engl J. Med. 2009, 361-1139-1151, Patel, et. al. N Engl J. Med. 2011, 365 883-891, Granger, et. al. N Engl J. The NOACs are primarily responsible for this, as they target proteins that are necessary for normal coagulation. Unmet needs in the prevention and treatment of thrombotic disorders or diseases are therefore novel therapies with improved safety profiles.
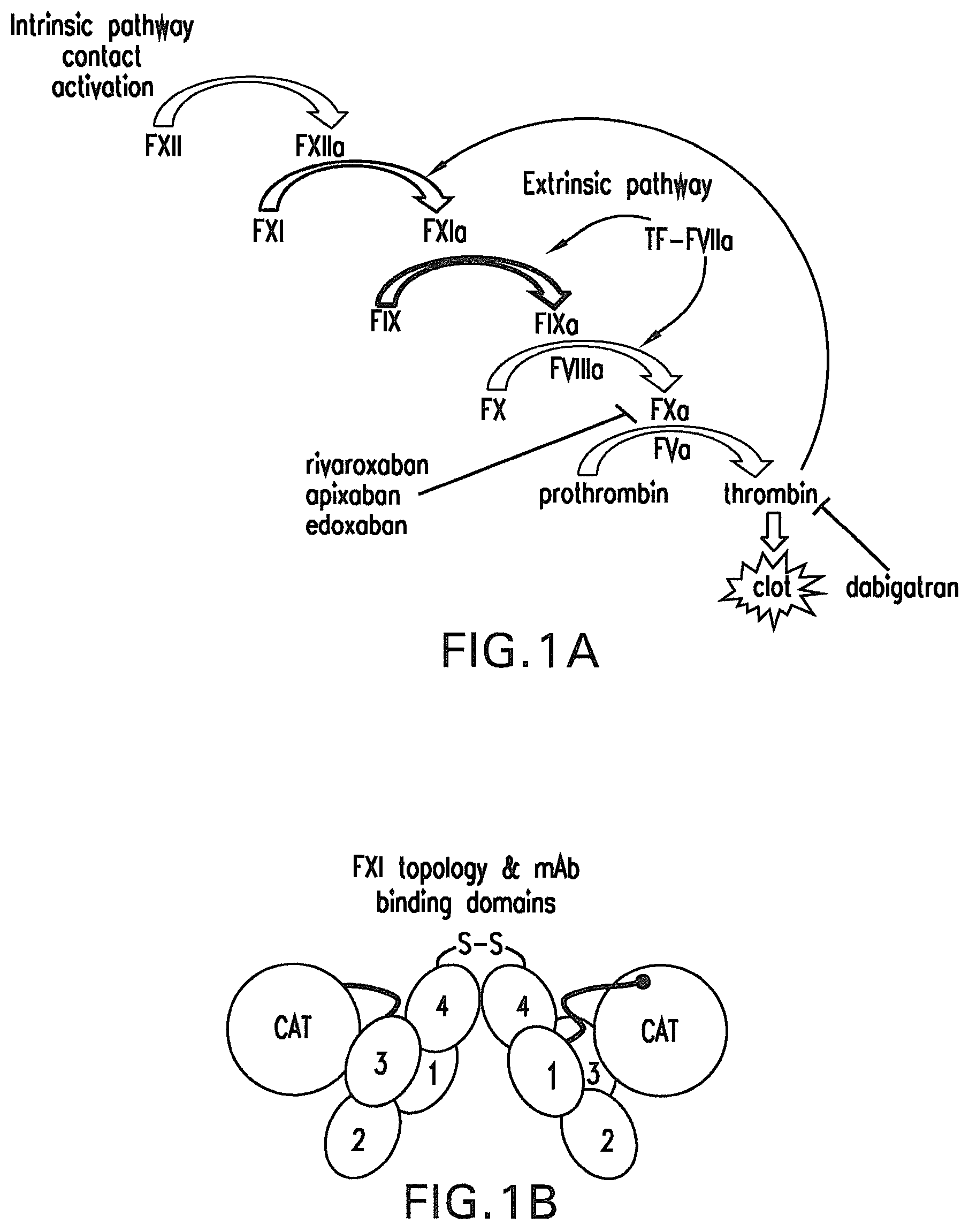
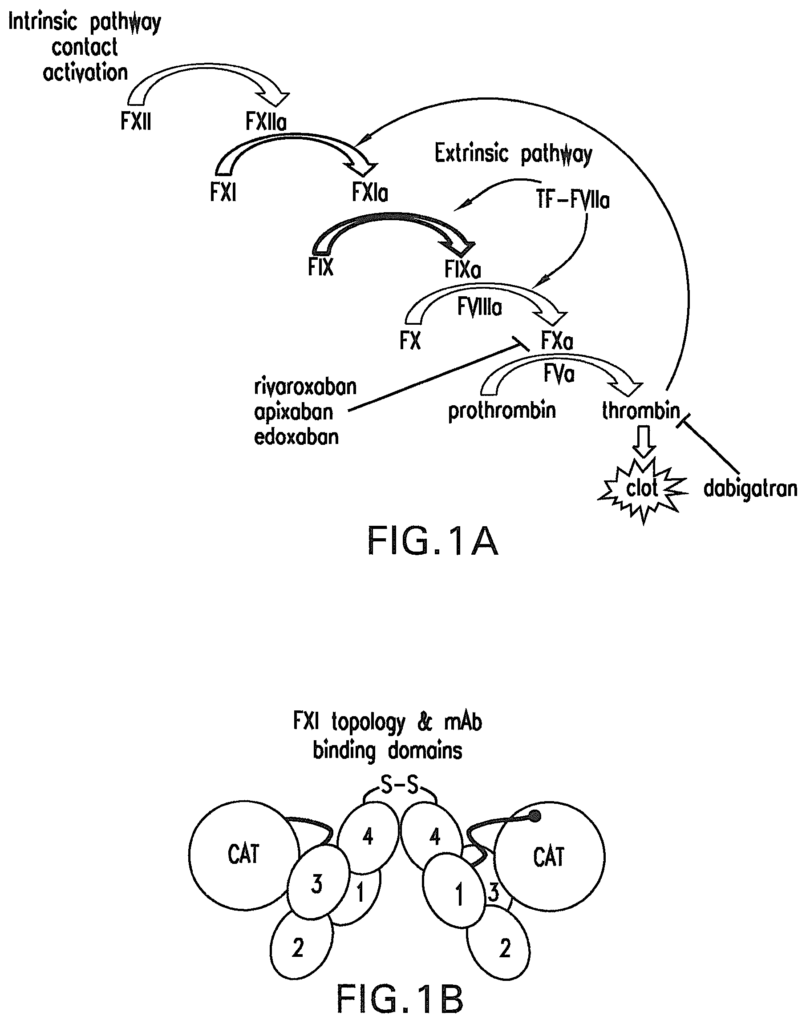
The classic waterfall model (FIG. In Figure 1A, coagulation can be triggered either by the extrinsic pathway (tissue factors (TF) activated) or the intrinsic pathway (contact-activated), both of which feed into the common pathway leading to thrombin production and fibrin (Furie & Furie Cell 1988,53:505-518, Gailani & Renne J Thromb Haemost 2007 5:1106-1112). Extrinsic cascades are initiated when TF, which is found in subendothelium or atherosclerotic lesion, is exposed to flowing blood. It then forms a complex with Coagulation Factor VIIa. The TF/FVIIa (extrinsic tenase) complex then triggers the ‘common pathway,’ i.e. FX is activated to form FXa, which then converts prothrombin into thrombin. The TF/FVIIa complex is also able to activate coagulation factor IX (FIX), forming FIXa. FIXa can also cleave FX substrate when it is in complex with coagulation factor VIII (FVIIIa). The intrinsic cascade begins when FXIIa forms via contact activation of negatively charged surfaces (e.g. Collagen and glycosaminoglycans propagate thrombin production by sequential activation FXI and FIX. As the terminal protease in the clotting process, thrombin may also contribute to FXIa formation by activating FXI directly in a feedback system. Platelets, an important component of whole blood that is activated by the thrombin, may also support FXIa. FXI-dependent amplification may regulate fibrinolysis indirectly via activation the thrombin activated fibrinolysis inhibit (TAFI). FXI interacts with multiple components of the hemostatic system, and plays a key role in blood coagulation (Gailani & Renne op. cit. ; Emsley et al., Blood 2010, 115:2569-2577).
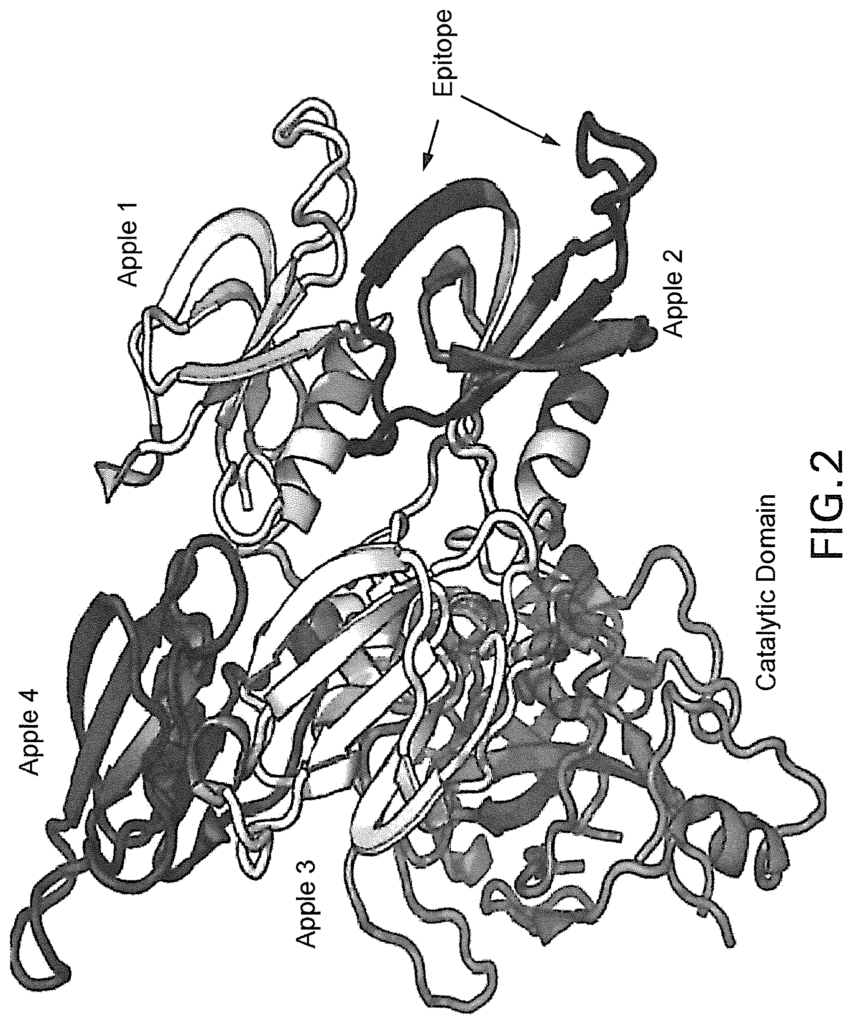
Coagulation Factor XI is a dimer consisting of identical subunits of 80 KDa. Each subunit, starting at the N-terminus, consists of four apple regions (A1, A2, and A3) and a catalytic region (See FIG. 1B). FXI circulates as a zymogen in complex with High Molecular weight Kininogen (HK). HK binds the A2 domain of FXI, and is a cofactor in activating FXI into FXIa by FXIIa. FXI’s remaining apple domains also play a role in important physiological functions. The FIX-binding domain is located in A3, while the FXIIa binding site is in A4. The residues critical for FXI dimerization can also be found in A4 by Emsley et. al. cit.).
The following key data support this notion: (1) in Ionis Pharmaceuticals Inc. FXI antisense oligonucleotide (ASO) Phase II trial (Buller et al., N Engl J Med 2015, 372:232-240), FXI ASO produced significant reduction in venous thromboembolism (VTE), with a trend toward less bleeding, compared to enoxaparin, among patients undergoing total knee arthroplasty; The following data supports this idea: (1) In Ionis Pharmaceuticals Inc. FXI Antisense Oligonucleotide Phase II Trial (Buller, et. al. N Engl J Medicine 2015, 372, 232-244), FXI ASO caused a significant reduction in venous embolism (VTE) with a tendency toward less bleeding compared to patients undergoing total joint arthroplasty. (2) Human Genetics and Epidemiological Studies (Duga, Semin
Chen, et. al., Drug Discov Today, 2014; Key, Hematology Am Soc Hematol Educ Program, 2014, 2014:66-70), indicated that severe FXI deficiencies (hemophilia A) confer a reduced risk of ischemic thrombosis and deep vein thrombosis. Conversely, higher levels of FXI were associated with an increased risk for VTE, ischemic thrombosis, and stroke. (3) Numerous pre op. cit.). Note that monoclonal antibody 14E11 and antigen 1A6 significantly reduced thrombus in the baboon model of AV shunt (U.S. No. 8,388,959; Tucker et al., Blood 2009, 113:936-944; Cheng et al., Blood 2010, 116:3981-3989). Transl Stroke Res, 2012, 3(3):381-389, Leung et. al.). Other FXI-targeting mAbs were also reported in preclinical studies that validate FXI’s antithrombotic potential with minimal bleeding risks (van Montfoort et. al. Thromb Haemost 2013 110; Takahashi et. al. Thromb Res 2010 125:464-4470; van Montfoort Ph.D. Thesis University of Amsterdam Amsterdam, Netherlands 14 Nov. 2014. The inhibition of FXI offers a novel antithrombotic treatment with a better benefit-risk ratio than current anticoagulants.
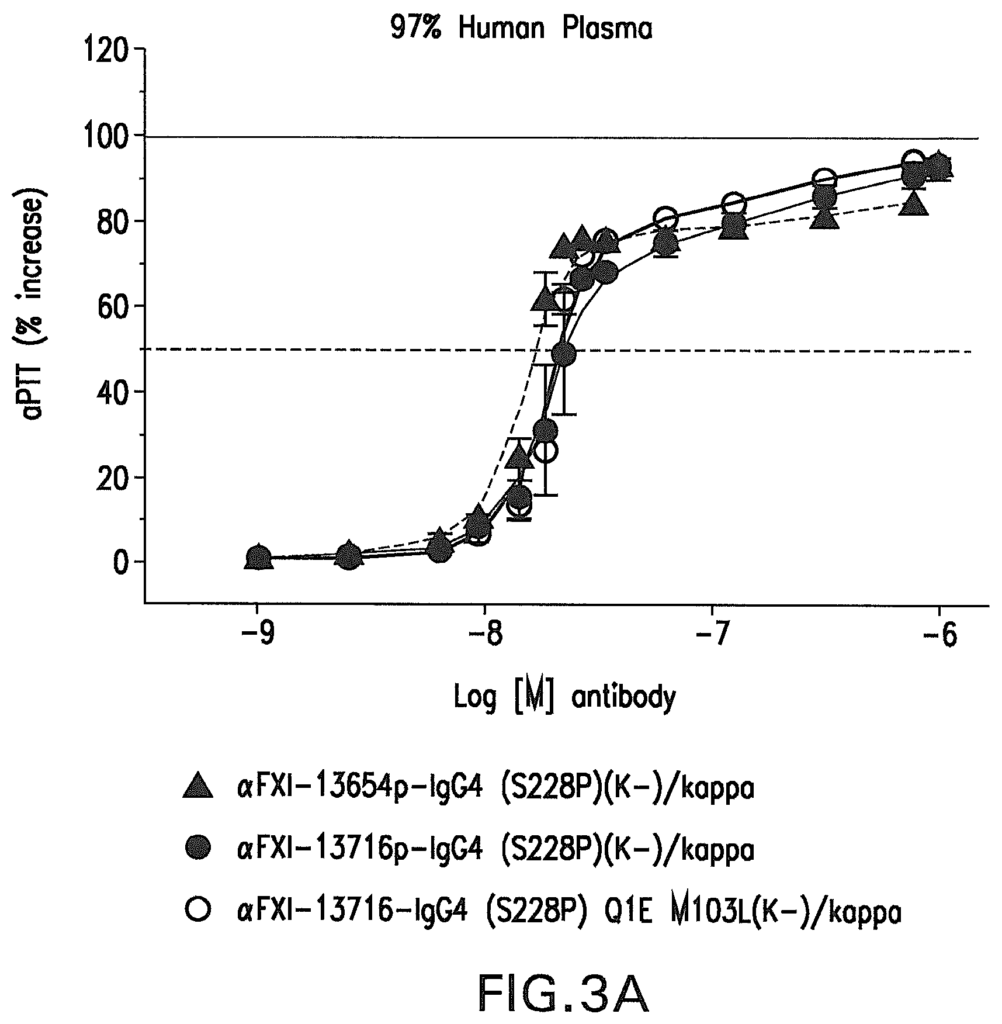
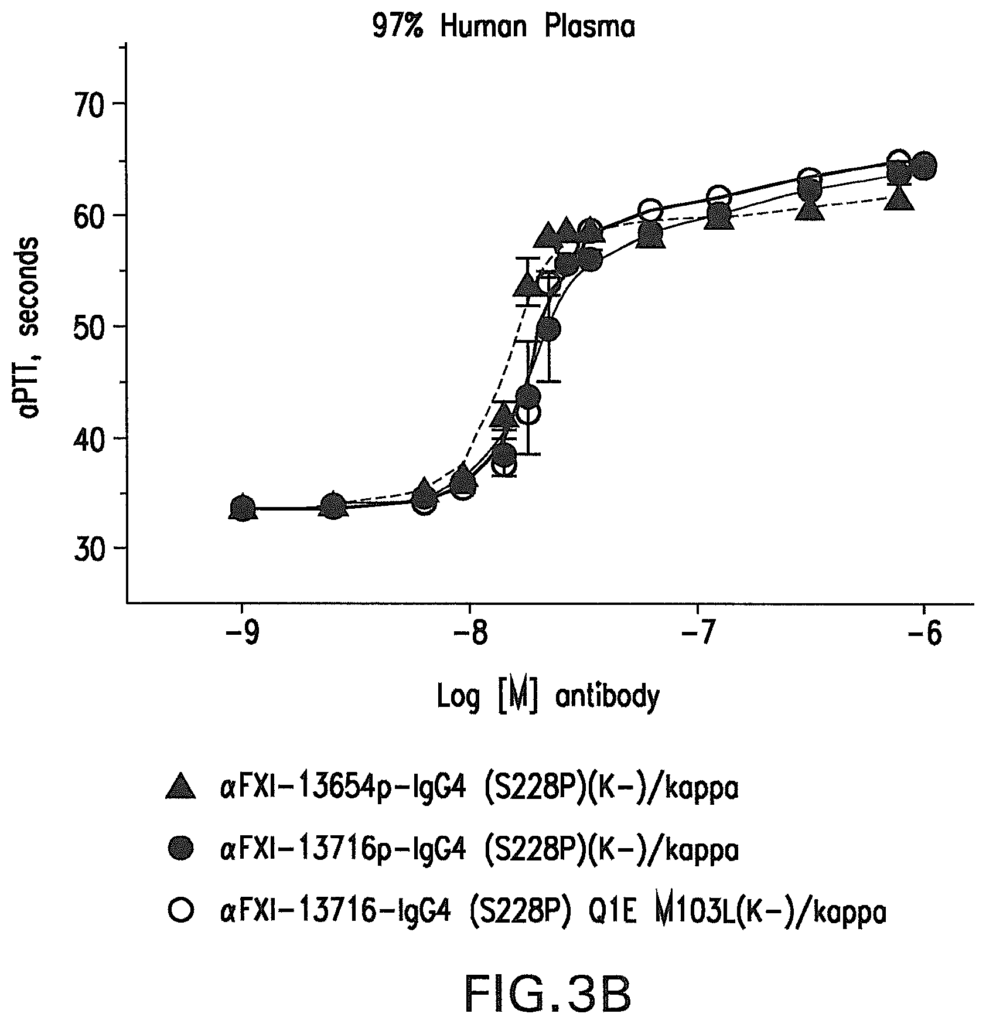
The present invention provides anti-FXI antibodies that can bind to coagulation factor XI and inhibit blood coagulation without compromising hemostasis. Preferably, the antibodies reduce blood clotting, associated thrombosis and induce little or no detectable blood bleeding. Anti-coagulation Factor XI antigens and antibodies are included in compositions that bind to a defined apple 2 domain epitope. These antibodies and antigen-binding fragments have neutralizing activity, inhibiting the conversion from the zymogen to activated form of coagulation factors XI, coagulation factor XIa via coagulation FXIIa.
The antibodies and antigen-binding fragments can be used for the treatment or prevention of thrombotic diseases and disorders. This includes but is not limited to myocardial ischemia, ischemicstroke, pulmonary and venous thromboembolisms, atrial fibrillation and disseminated intervascular coagulation. The antibodies and antigen-binding fragments are especially useful for Stroke Prevention in Atrial Fibrillation.
The present invention provides an antigen or antibody binding fragment that comprises at least six complementarity-determining regions (CDRs), of antibodies?FXI 13654p or -13716p or AD-13716p or -13716, respectively, and where one or two of these CDRs have one, two or three amino acids substitutions or additions or combinations of amino acids, and where antibody ‘FXI 13654p’ comprises a heavy-chain (HC) with the amino-
The present invention provides an antigen or antibody binding fragment that comprises at least six complementarity-determining regions (CDRs), of antibodies ‘FXI 13654p or AD-13716p or at least six CDRs from antibody ‘FXI 13716p or -13716. This includes an HC with the amino sequence of SEQ NO:22, 33 or 34 and a
In further embodiments, the six CDRs include CDR1,CDR2,and CDR3 from the HC of antibodies?FXI13654p?FXI13716p?or?FXI13716?and CDR1,CDR2,and CDR3 from the LC of these antibodies?FXI13654p?FXI13716p?or?FXI13716?. The six CDRs in further embodiments include CDR1,CDR2,and CDR3 from the HC of antibodies ‘FXI13654p or ‘FXI13716p or a combination thereof. One or more CDRs may have one,two,orthree amino acid modifications, additions or deletions.
The antibody or antigen-binding fragment may also include: (i) HC CDRs with amino acids sequences SEQ NO :1, SEQ NO :2, SEQ NO :3, and SEQ NO :4 for HC CDR1, CDR2 or CDR3 and LC CDRs
The antibody or antigen-binding fragment may also include (i) HC CDRs with amino acids sequences as set out in SEQ NO.1, SEQ NO.2, and SEQ NO.3 and LC CDRs with amino acids sequences as set out in SEQ NO.7,SEQ NO.8, andSEQ NO.9, and LC CDRs that have aminos sequences in SEQ NO.10,SEQ NO.11, and
The antibody or antigen-binding fragment may also include CDR1,CDR2,and CDR3 from the HC domain of antibody FXI-1371p in a variable HC domain with the amino acids shown in SEQ NO:16, for antibody FXI-1371p and SEQ NO:24, for antibody FXI 13716, and CDR1,CDR2,and CDR3 from the LC domain of antibody,FXI-1354p in a variable LC domain, which has the same as SEQID NO:
In other aspects or embodiments of this invention, the antigen comprises a constant domain HC comprising the amino acids shown in SEQ NO:14 or No.40 or variants thereof, in which the constant contains 1, 2, 3, 4, 6, 7, 8, 9 or 10 amino acid additions, deletions or combinations thereof.
In other aspects or embodiments of this invention, the antigen comprises a LC domain consisting of the amino acid sequence SEQ ID No:15, or a variant thereof, in which the constant region contains 1, 2, 3, 4, 6, 7, 8, 9 or 10 amino acids substitutions, additions or deletions.
The present invention also provides an antigen or antibody binding fragment that contains at least six complementarity-determining regions (CDRs), whereby antibody ‘FXI 13654p has a heavy-chain (HC) with the amino-acid sequence shown on SEQ NO:18, 26, 31 or 32, and a lighter-chain (LC) with the sequence shown on SEQ NO:19, and whereby antibody ‘FXI 13716p includes an HC showing the sequence of amino-a
The HC and LC CDRs for antibody FXI 13716p contain the amino acids sequences in SEQ NO :7 and SEQ NO :8 and SEQ NO :9, while the LC and CDRs are the amino acids sequences in SEQ NO :10 and SEQ NO :11 and 12 respectively. Optionally, one or two of the CDRs may have one, three, or four amino acid additions or deletions.
The?FXI 13654p antigen comprises an amino-acid sequence of SEQ NO:16 in an HC-variable domain and an amino-acid sequence of SEQ NO:17 in an LC-variable domain, with optionally 1, 2, 3 amino-acid substitutions or additions or deletions in either or both variable-domains. In a second embodiment, one, two, or three amino acids can be substituted, added, deleted, or combined in the framework region of the aforementioned HC and LC variable regions.
Click here to view the patent on Google Patents.
Leave a Reply