Invented by Brian Wong, Julie Hambleton, Robert Sikorski, Emma Masteller, Kevin Hestir, David Bellovin, Katherine E. Lewis, Bristol Myers Squibb Co, Five Prime Therapeutics Inc
Anti-CSF1R (Colony-Stimulating Factor 1 Receptor) antibodies work by blocking the CSF1R pathway, which is responsible for promoting the growth and survival of tumor-associated macrophages (TAMs). TAMs are immune cells that infiltrate the tumor microenvironment and play a crucial role in promoting tumor growth, angiogenesis, and immunosuppression. By inhibiting the CSF1R pathway, anti-CSF1R antibodies effectively deplete TAMs, thereby weakening the tumor’s ability to evade the immune system.
On the other hand, anti-PD-1 (Programmed Death-1) antibodies target the PD-1 pathway, which is involved in regulating T-cell responses. Tumors often exploit this pathway by expressing PD-L1 (Programmed Death-Ligand 1), a protein that binds to PD-1 receptors on T-cells, leading to T-cell exhaustion and immune evasion. Anti-PD-1 antibodies block this interaction, reinvigorating the immune response against cancer cells.
Combining these two therapies has shown promising results in preclinical and clinical studies. By simultaneously targeting TAMs and reactivating T-cell responses, the combination therapy enhances the overall anti-tumor immune response. This approach has demonstrated improved tumor regression rates, prolonged survival, and increased response rates compared to single-agent therapies.
One example of the potential of this combination therapy is in the treatment of certain types of solid tumors, such as melanoma and non-small cell lung cancer (NSCLC). These cancers often exhibit high levels of TAM infiltration and PD-L1 expression, making them ideal candidates for this dual-targeted approach. Clinical trials investigating the combination of anti-CSF1R and anti-PD-1 antibodies in these cancers have shown promising results, with some patients experiencing complete or partial tumor regression.
The market for combination therapy of anti-CSF1R and anti-PD-1 antibodies is expected to grow significantly in the coming years. Several pharmaceutical companies are actively developing and testing these therapies, aiming to gain regulatory approval and bring them to market. The potential market size for these therapies is substantial, considering the prevalence of cancers that could benefit from this approach.
However, challenges remain in the development and commercialization of combination therapies. Identifying the optimal dosage, treatment schedule, and patient selection criteria are crucial for maximizing the therapeutic benefits. Additionally, the high cost of these therapies may pose a barrier to widespread adoption, especially in healthcare systems with limited resources.
In conclusion, the market for combination therapy of anti-CSF1R and anti-PD-1 antibodies for certain cancers holds great promise in revolutionizing cancer treatment. This innovative approach has the potential to significantly improve patient outcomes by enhancing the anti-tumor immune response. As further research and clinical trials continue to validate the efficacy and safety of these therapies, the market is expected to grow, offering new hope for patients with cancers that have been historically challenging to treat.
![]()
The Bristol Myers Squibb Co, Five Prime Therapeutics Inc invention works as follows
The combination of PD-1/PD-L1 and antibodies that bind to colony stimulating factors 1 receptor (CSF1R), in combination with PD-1/PD-L1 inhibitors, is a method for treating cancer.
Background for Combination therapy of anti-CSF1R and anti-PD-1 antibodies for certain cancers
The “Colony Stimulating Factor 1 Receptor” (also referred to as CSF1R, also known in the art by FMS, FIM2, CFMS, M CSF receptor and CD115) consists of a single-pass, transmembrane, receptor with an extracellular domain at its N-terminus and a C terminal intracellular domain that has tyrosine-kinase activities. CSF1 and the interleukin 34 ligand, (referred to as IL34 herein; Lin et. al., Science 320, 807-11 (2008)), bind to CSF1R, causing receptor dimerization. This leads to an increase in CSF1R protein tyrosine kinase activities, phosphorylation at CSF1R tyrosine residua, and downstream signaling. CSF1R activation leads to the survival, proliferation and differentiation of macrophages and monocytes as well as other monocytic cells such as osteoclasts.
Many tumor cells and tumor stromal cell have been shown to produce CSF1, activating monocyte/macrophages cells via CSF1R. It has been demonstrated that the amount of CSF1 found in tumors correlates with the number of tumor-associated macacaphages. In most cancers, higher levels of TAMs correlate with a worse prognosis. CSF1 was also found to promote tumor progression and growth in human breast cancer mouse xenografts. See, e.g., Paulus et al., Cancer Res. 66: 4349-56 (2006). CSF1R also plays a part in osteolytic bone degradation in bone metastasis. See, e.g., Ohno et al., Mol. Cancer Ther. 5: 2634-43 (2006). TAMs promote tumour growth in part by suppressing antitumor T-cell effector function via the release of immunesuppressive molecules and the expression T cell inhibitory surfaces proteins.
Genetic changes in cancer can provide a variety of antigens which mediate antitumor immunity. T-cell responses are initiated by TCR recognition of antigens. This is regulated through a balance of activating and inhibiting signals. The inhibitory signal, or “immune-checkpoints”, is what regulates T-cell responses. Normal tissues play a key role in preventing autoimmunity. Cancers can evade antitumor immunity by up-regulating immune checkpoint protein. Two immune checkpoint proteins have been the focus of clinical cancer immunotherapeutics, cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed cell death protein 1 (PD-1). Combining an anti CTLA-4 antibody with an anti PD-1 antibody was approved to treat metastatic melanoma. Several additional clinical trials have been conducted to investigate the use of the combination in the treatment other cancers. Clinical trials are currently studying anti-PD-1 and anti-CTLA-4 monotherapies as a treatment option for various types of cancer. Anti-PDL1 antibodies, which bind PD-1 ligand PD-L1, are currently being developed in the clinic.
The combination of anti-CTLA-4 antibody (anti-CTLA-4 Ab) and an anti-PD-1 antibody (anti PD-1 Ab) has shown improved overall response rates, increased complete response rates, as well as overall survival rates in metastatic melanoma, compared to the use of only anti CTLA-4 ab. Initial clinical results showed that the combination of anti-CTLA-4 antibodies (anti CTLA-4 Ab) with anti-PD-1 antibodies (anti PD-1 Ab), demonstrated better overall response rates and complete response rates as well as improved overall survival rates for metastatic melanoma compared to anti CTLA-4 ab alone or historical control.
As described herein, clinical trials have demonstrated significant antitumor activities of an anti PD-1 antibody combined with an anti CSF1R antibodies.
In certain embodiments, cancer treatment methods are provided. The method comprises administering an anti-CSF1R antibody and a PD-1/PD-L1 inhibitor to the subject. In some embodiments the PD/PD-L1 inhibitor is an antibody. In some embodiments the PD-1/PD-L1 is an anti-PD-1 antibodies. In certain embodiments, an anti-PD-1 antibodies consists of the heavy and light chain CDRs from an antibody selected between nivolumab or pembrolizumab. In some embodiments the anti-PD-1 antibodies comprises the heavy and light chain variable region of an antibody chosen from nivolumab or pembrolizumab. In certain embodiments, anti-PD-1 antibodies are selected from nivolumab or pembrolizumab. In some embodiments the PD-1/PD-L1 inhibitor is an anti PD-L1 antibodies. In some embodiments the anti-PDL1 antibody consists of the heavy and light chain CDRs from an antibody selected among BMS-936559 MPDL3280A MEDI4736 and MSB0010718C. In some embodiments the anti-PDL1 antibody consists of the heavy chain and the light chain variable region of an antibody chosen from BMS-936559 MPDL3280A MEDI4736 and MSB0010718C. In certain embodiments, anti-PDL1 antibodies are selected from BMS-936559 MPDL3280A MEDI4736 and MSB0010718C. In some embodiments the PD-1/PD-L1 is a fusion. In some embodiments the fusion is AMP-224.
In some embodiments the anti-CSF1R and the PD-1/PD-L1 inhibitor are administered simultaneously or sequentially. In certain embodiments, both the anti-CSF1R and the PD-1-PD-L1 inhibitor are administered simultaneously. In some embodiments one or more doses are given of the PD/PD-L1 before administering anti-CSF1R antibodies. In some embodiments the subject has received a full course of PD/PDL1 inhibitor therapy before receiving the anti-CSF1R antibodies. In some embodiments the anti-CSF1R is administered as part of a second course PD-1/PDL1 inhibitor therapy. In some embodiments the subject received one, two, three or four doses of PD-1/PDL1 inhibitor before the anti-CSF1R was administered. In certain embodiments, the anti-CSF1R antibody is administered in conjunction with at least one dose. In some embodiments one or more anti-CSF1R antibodies are administered before administering a PD-1-PD-L1 inhibitor. In some embodiments the subject received two, three, four, or five doses of anti-CSF1R before the PD-1/PD-L1 inhibitor was administered. In certain embodiments, the anti-CSF1R is administered simultaneously with the PD-1/PD-L1 inhibitor. In some embodiments the two drugs may be administered at the same time. In some embodiments the drugs are combined prior to administration, and administered as mixtre. In some embodiments the drugs can be stored and packaged in the same vial, or vials with each drug separately may be mixed just before administration. The drugs can be administered by various routes in various embodiments. These include, but are not limited to: oral, intra-arterial parenteral intranasal intravenous intraventricular intracardiac buccal rectal intraperitoneal intratracheal intraperitoneal intraperitoneal intradermal topical transdermal intrathecal.
In some embodiments, anti-CSF1R antibodies are administered at doses of about 0,1, about 0.3, or 0.5 mg/kg. In some embodiments the PD-1/PD-L1 is administered in a dose ranging from 0.1-10mg/kg. For example, about 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10mg/kg. In some embodiments the anti-CSF1R and the PD/PD-L1 inhibitor are administered at one of the doses above, about once every 1, 2, 3, 4 or 5 weeks.
In certain embodiments the first dose is therapeutic and the second is therapeutic. In some embodiments, the subtherapeutic first dose and therapeutic second dose are used. In some embodiments the first dose can range from 80 mg up to 800 mg, or 0.1 mg/kg and at least 10.0 mg/kg. In some embodiments the second dose can range from 80 mg up to 800 mg, or 0.1 mg/kg up to 10.0 mg/kg. In one embodiment, the first dosage is given at a dosage of at least 3 mg/kg or 240mg once every two weeks.
In some embodiments the subject receives at minimum two doses. At least three doses. At least four doses.
In some embodiments the first dose can be a flat or weight-based dose. In some embodiments, the second dosage is a weight-based dose or a flat dose.
In some embodiments, cancers selected include non-small cell lungs cancer, melanoma (including squamous cells), squamous carcinomas of the head and throat, pancreatic, renal, cell, carcinomas, endometrial, and hepatocellular cancer. In some embodiments the cancer is central nervous system tumour. In some embodiments the central nervous system tumor is a malignant tumour such as glioblastoma. In some embodiments the cancer is recurrent after surgery, chemotherapy or radiation therapy or a combination of these therapies. In certain embodiments, the cancer is stage III or IV, as described in the section below on specific cancers. In some embodiments the cancer of the patient is metastatic. In some embodiments the subject is a PD-1/PD-L1 insufficient responder or is refractory prior treatment with a PD-1/PD-L1 antagonist. In some embodiments the patient has received PD/PDL1 inhibitor treatment, while in others the subject did not receive PD/PDL1 inhibitor treatment. In some embodiments the subject has received chemotherapy, radiation therapy or surgery. In other embodiments, there is documented tumor progression despite prior treatment. In some embodiments the anti CSF1R and PD-1-PD-L1 inhibits have a synergistic impact on tumor growth and weight in a mouse xenograft cancer model compared to the anti CSF1R or PD-1-PD-L1 alone.
In certain embodiments, a patient with non small cell lung cancer is treated with an anti CSF1R (for example, an anti CSF1R as described herein such as an anti antibody comprising both the heavy and light chains CDRs from HuAB1), and a PD-1/PD-L1 (for example, an anti PD-1 antibody comprising heavy chain and lighter CDRs from nivolumab, pembrolizumab, or a PD-1/PD-L1 fusion protein or peptide or fusion protein a PD a PD1 a PD1 PD1 PD1 PD1 PD1 PD1 PD-1/PD1 PD1 PD1 PD1 PD1 PD-1 a PD PD-L1 PD-L1 PD-L1 PD-L1-L1-L1-L1-1/PD fusion protein or peptide or fusion proteins or PD-1/PD -2/PD-1/PD-2/PD-2/PD-2/PD-2 -2/PD-1/PD-22/AMP-224 or In some embodiments, a patient with advanced or metastatic cancer has Stage IIIB or Stage IV disease. The patient may also have demonstrated progression of disease or recurrence after or during a platinum-dodecylated or other chemotherapy regimen. In some embodiments the patient had not been exposed to a PD-1/PD-L1 antagonist before, while in other embodiments the patient was refractory. In some embodiments the anti-CSF1R is administered in a dose between about 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10 mg/kg. In some embodiments the PD-1/PD-L1 is administered in a dosage of 0.1-10mg/kg. For example, 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10mg/kg. In some embodiments the anti-CSF1R and PD-1/PDL1 inhibitors are administered at one of the doses above, once every 1, 2, 3, 4 or 5 weeks. For example, about once every two weeks. In some embodiments the anti CSF1R and PD-1/PDL1 inhibitors have a synergistic impact on tumor growth, volume, and/or weight in a mouse xenograft NSCLC model compared to the anti CSF1R or PD 1/PDL1 inhibitors alone.
In certain embodiments, melanoma can be treated with an anti CSF1R (for example, an antibody comprising heavy chain and CDRs light of HuAB1), and PD-1/PDL1 inhibitors (for example, an anti PD-1 antibody comprising heavy chain and CDRs light of nivolumab, or pembrolizumab, or a PD-1/PD-L1 fusion protein, peptide, or AMP-224, or a In some embodiments, a patient with Stage III or Stage IV melanoma is treated. In some embodiments the patient is BRAF-wild type or has shown disease progression after or during treatment with atleast one BRAF inhibitor. In some embodiments the patient had not been exposed to a PD-1/PD-L1 antagonist before, while in other embodiments the patient was refractory. In some embodiments the anti-CSF1R is administered in a dose between about 0.1 and about 0.3 mg/kg. In some embodiments the PD-1/PD-L1 is administered in a dosage of 0.1-10mg/kg. For example, 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10mg/kg. In some embodiments the anti-CSF1R and PD-1/PDL1 inhibitors are administered at one of the doses above, once every 1, 2, 3, 4 or 5 weeks. For example, about once every two weeks. In some embodiments the anti CSF1R and PD-1/PDL1 inhibitors have a synergistic impact on tumor growth, volume, or weight in a mouse xenograft melanoma model compared to the anti CSF1R and PD/PD-L1 alone.
In some embodiments, squamous-cell carcinoma of the neck and head (SSCHN), is treated with an anti CSF1R (for example, an antibody comprising heavy and light chains CDRs from HuAB1), and a PD-1/PD-L1 (for example, an anti PD-1 antibody comprising heavy chain and heavy-chain CDRs from nivolumab, or pembrolizumab, or a PD-1/PD-L1 fusion protein or peptide fusion protein or peptide fusion AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-1/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AMP-2/AUR-012 or fusion protein or aUR-012 or peptide or peptide or fusion-protein or NP-224 or aUR-012, such as aUR-012 or AUR-012 or aUR-012 In some embodiments the patient has Stage III, IV or metastatic SSCHN. In some embodiments the patient may have previously received platinum therapy or chemotherapy but still demonstrated tumor progression. In some embodiments the patient may have received platinum therapy and/or radiation therapy in combination, but tumor progression or recurrence has been demonstrated. In some embodiments the patient has never been exposed to a PD-1/PD-L1 antagonist, while in other embodiments the patient is refractory. In some embodiments the anti-CSF1R is administered in a dose between about 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10 mg/kg. In some embodiments the PD-1/PD-L1 is administered in a dosage of 0.1-10mg/kg. For example, 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10mg/kg. In some embodiments the anti-CSF1R and PD-1/PDL1 inhibitors are administered at one of the doses above, for example once per 1, 2, 3 or 4 weeks. In some embodiments the anti CSF1R and PD-1/PDL1 inhibitors have a synergistic impact on tumor growth, volume, weight and/or weight in a mouse xenograft for squamous-cell carcinoma compared with administration of either the anti CSF1R or PD 1/PD L1 inhibitors alone.
In certain embodiments, pancreatic carcinoma is treated with an anti CSF1R (for example, an anti CSF1R as described herein such as an antibodies comprising the light and heavy chain CDRs from HuAB1), and the PD-1/PD-L1 (for example, an anti PD-1 antibody comprising heavy chain and lighter chain CDRs from nivolumab, or pembrolizumab, or a PD-1/PD-L1 fusion protein In some embodiments the patient may have a documented adenocarcinoma or metastatic pancreas. In some embodiments the patient has received radiation or surgery in the past. In some embodiments the patient had not been exposed to a PD-1/PD-L1 inhibitor before, while in others the patient was refractory. In certain embodiments, anti-CSF1R antibodies are administered at doses of 0.1 to 0.3 mg/kg. In some embodiments the PD-1/PD-L1 is administered in a dosage of 0.5-10mg/kg. For example, 1, 2, 3, 4 or 5mg/kg. In some embodiments the anti-CSF1R and PD-1/PDL1 inhibitors are administered at the doses above, for example, once every 1, 2, 3, 4 or 5 weeks. In certain embodiments, colorectal carcinoma is treated using the anti-CSF1R (for example, an antibody comprising both the heavy chain CDRs and light chains of HuAB1), and the PD/PD-L1 inhibit (for example, an anti PD-1 antibody comprising heavy chain CDRs and light chains of nivolumab, pembrolizumab, or a PD/PD-L1 fusion protein, peptide, or AMP-224, or AUR-012 or a AMP-2/AUR-012 In some embodiments the patient has an adenocarcinoma in the colon or rectum. In certain embodiments, the cancer is metastatic. In some embodiments the patient has metastatic cancer despite having received prior treatment, including fluoropyrimidine or oxaliplatin or irinotecan or bevacizumab or cetuximab or panitumumab. In some embodiments the patient had not been exposed to a PD-1/PD-L1 antagonist before, while in other embodiments the patient was refractory. In some embodiments the anti-CSF1R is administered in a dose between about 0.1 and about 10 mg/kg. In some embodiments the PD-1/PD-L1 is administered in a dosage of 0.1-10mg/kg. For example, about 0.1, 0.3, 0.5, 1, 2, 3, 4, 5, or 10mg/kg. In some embodiments the anti-CSF1R and PD-1/PDL1 inhibitors are administered at a dose of 0.1-10 mg/kg, for example, about 0.1, about 0.3, about 0.5, approximately 1, approximately 2, approximately 3, approximately 4, or roughly 5 mg/kg every 1, 2, 3, 4 or 5 weeks. In some embodiments the anti-CSF1R and PD-1/PDL1 inhibitors have a synergistic impact on tumor weight and/or size when compared to a mouse xenograft pancreatic cancer model (such as a KRasG12D/Ink4a??/? In some embodiments, administration of anti-CSF1R antibodies and PD-1/PDL1 inhibitors results in a synergistic effect on tumor growth, weight and/or volume compared with a mouse xenograft model for pancreatic cancer (such as a model comprising KRasG12D/Ink4a?/?
In some embodiments of the methods, malignant glioma (e.g. glioblastoma or gliosarcoma) is treated with the anti-CSF1R antibody (for instance, an anti-CSF1R antibody as described herein, such as an antibody comprising the heavy and light chain CDRs of HuAB1) and the PD-1/PD-L1 inhibitor (for instance, an anti-PD-1 antibody comprising the heavy chain and light chain CDRs of nivolumab or pembrolizumab or a PD-1/PD-L1 inhibitor fusion protein or peptide such as AMP-224 or AUR-012). In some embodiments, the patient has previously been treated with surgery, radiotherapy, and/or temozolomide. In some embodiments, the patient has Grade IV malignant glioma. In some embodiments, the patient has not had prior exposure to a PD-1/PD-L1 inhibitor, and in other embodiments, the patient is refractory to PD-1/PD-L1 inhibitor treatment. In some embodiments, the anti-CSF1R antibody is administered at a dose of about 0.1, about 0.3, about 0.5, about 1, about 2, about 3, about 4, about 5 or about 10 mg/kg. In some embodiments, the PD-1/PD-L1 inhibitor is administered at a dose of 0.1-10 mg/kg, such as, for example about 0.1, about 0.3, about 0.5, about 1, about 2, about 3, about 4, about 5 or about 10 mg/kg mg/kg. In some embodiments, the anti-CSF1R antibody and the PD-1/PD-L1 inhibitor are administered, for example at one of the above doses, once per 1, 2, 3, 4, or 5 weeks, such as about once every 2 weeks. In some embodiments, administration of the anti-CSF1R antibody and the PD-1/PD-L1 inhibitor results in a synergistic effect on tumor growth, weight, and/or volume compared in a mouse xenograft model for glioma compared to administration of the anti-CSF1R antibody or PD-1/PD-L1 inhibitor alone.
In some embodiments, administering additional anti-cancer drugs is also included in the method. In some embodiments, an anti-cancer drug is chosen from a group of antigens or antibodies that specifically bind to CTLA-4. The anti-CTLA-4 agent inhibits CTLA-4, chemotherapy, platinum-based doublet therapy, an inhibitor of VEGF, Indoleaminepyrrole 2,3,dioxygenase, IDO, or a combination thereof. The anti-cancer drug is ipilimumab in one embodiment.
In certain embodiments, compositions comprising an anti CSF1R antibody and a PD-1/PD-L1 inhibitor are provided.” In some embodiments the PD/PD-L1 is an anti-body. In some embodiments the PD-1/PD-L1 is an anti-PD-1 antibodies. In certain embodiments, an anti-PD-1 antibodies consists of the heavy and light chain CDRs from an antibody selected between nivolumab or pembrolizumab. In some embodiments the anti-PD-1 antibodies comprises the heavy and light chain variable region of an antibody chosen from nivolumab or pembrolizumab. In certain embodiments, anti-PD-1 antibodies are selected from nivolumab or pembrolizumab. In some embodiments the PD-1/PD-L1 inhibitor is an anti PD-L1 antibodies. In some embodiments the anti-PDL1 antibody is composed of the heavy and light chain CDRs from an antibody selected among BMS-936559 MPDL3280A MEDI4736 and MSB0010718C. In some embodiments the anti-PD-1 antibodies are the heavy chain and the light chain variable region of an antibody chosen from BMS-936559 MPDL3280A MEDI4736 and MSB0010718C. In certain embodiments, anti-PD-1 antibodies are selected from BMS-936559 MPDL3280A MEDI4736 and MSB0010718C. In some embodiments the PD-1/PD-L1 is a fusion. In some embodiments the fusion is AMP-224.
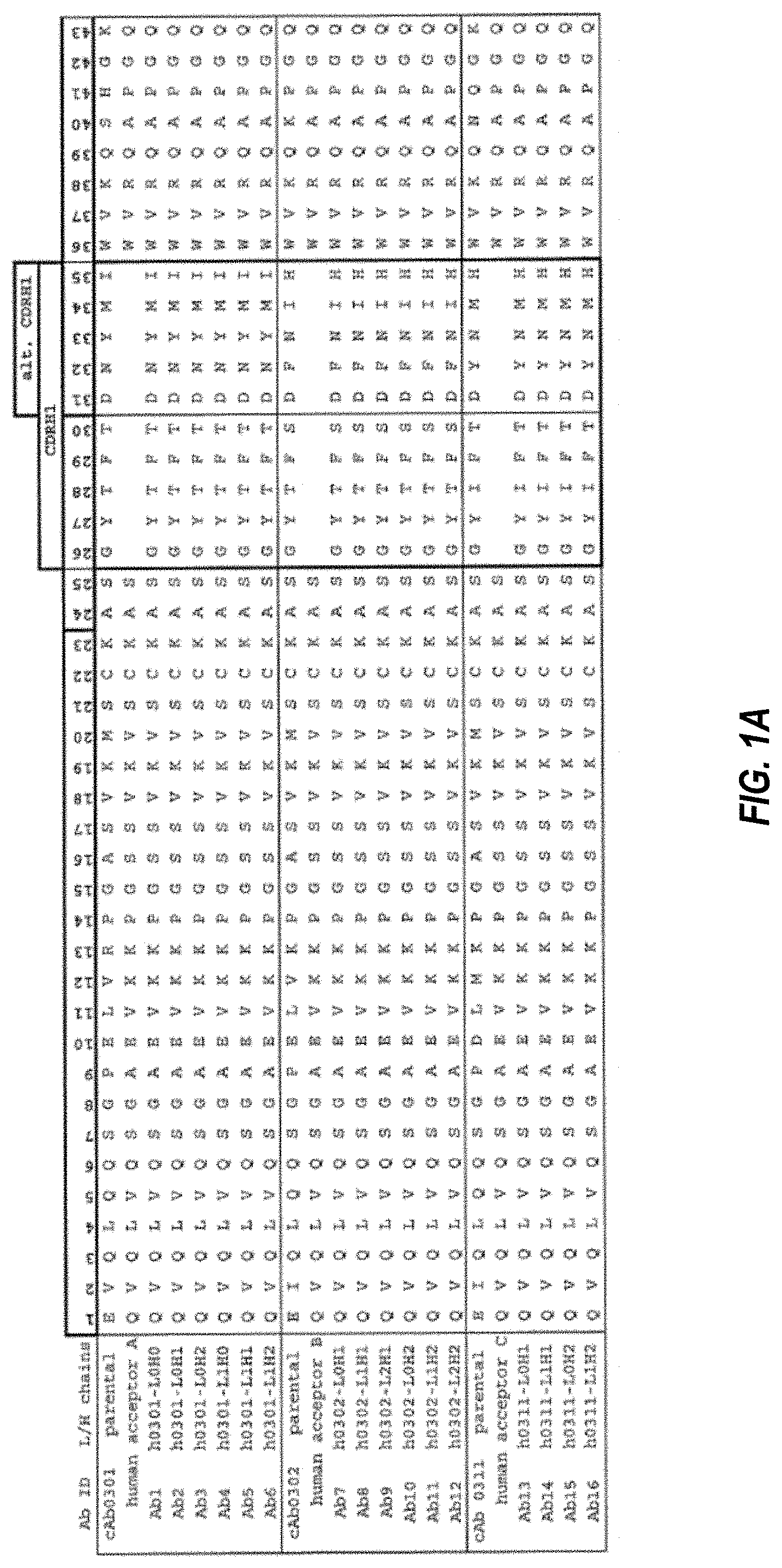
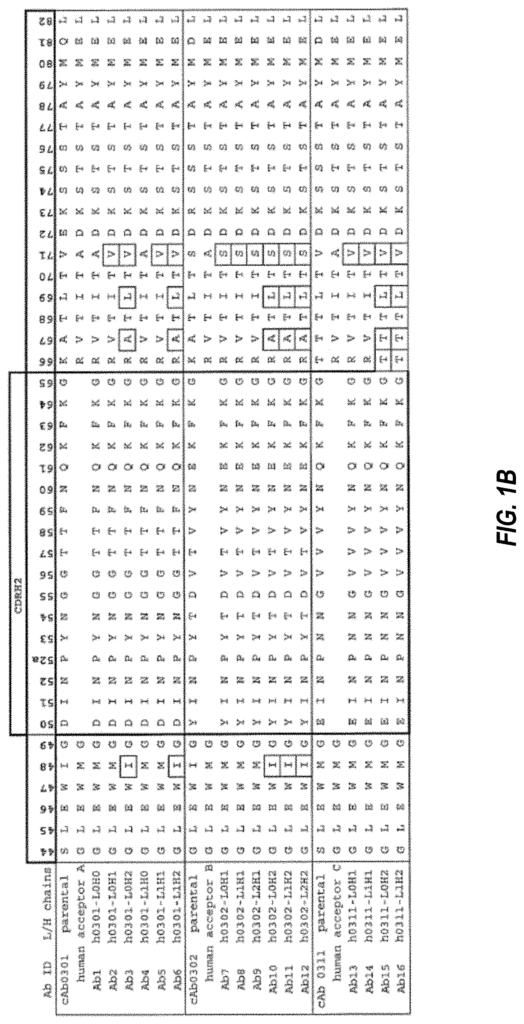
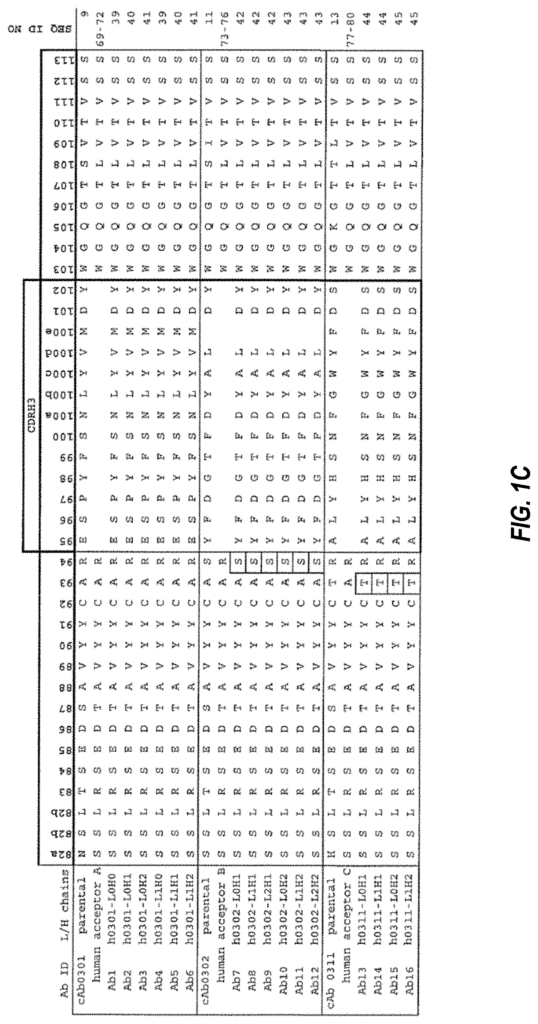
The anti-CSF1R antibodies heavy chain or light chain may be arranged as follows in any compositions or methods described.
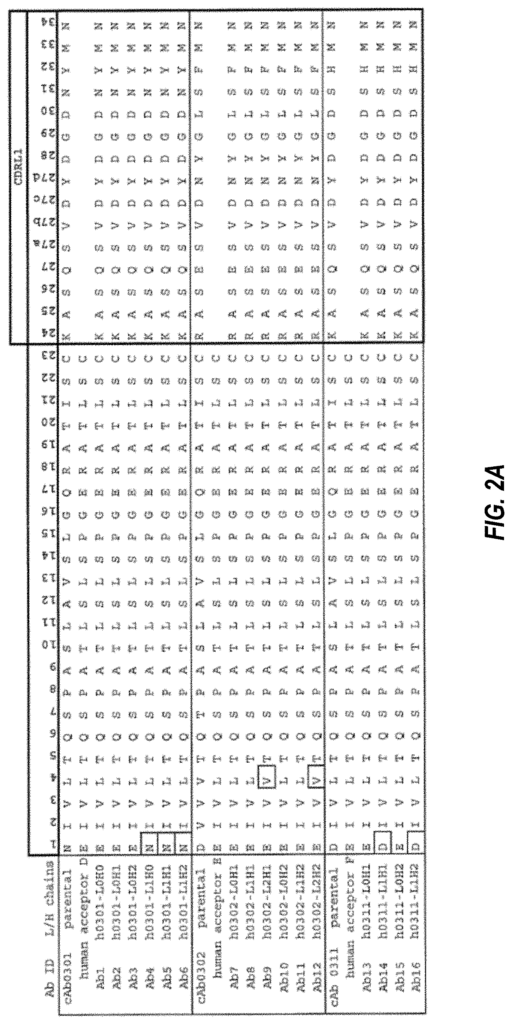
In any of the compositions and methods described in this document, the anti CSF1R heavy chain can contain a sequence which is at least 90% identical to one selected from SEQ NOs: 9, 11-13, and 39-45. In any of these methods, the anti CSF1R light chain can contain a specific sequence that is 90%, 95%, 97%, 99% or 100% identical to the sequences selected from SEQ NOs 10, 12, 14 and 46 to52. The anti-CSF1R heavy chain can be a combination of a minimum 90%, 95%, 97% or 100% sequence from SEQ NOs 9, 11, 13 and 39 to 44. The anti-CSF1R light chain is a 90%, 95% or 97% sequence from SEQ NOs 10, 12, 14 and 46 to52.
Click here to view the patent on Google Patents.
Leave a Reply