
Invented by Scott Koenig, Ronald L. Wilder, Ezio Bonvini, Leslie S. Johnson, Provention Bio Inc
![]()
The Provention Bio Inc invention works as follows
The present invention provides methods for treating, preventing or slowing down the progression of immunological diseases mediated by T cells, especially autoimmune diseases. Type 1 diabetes (also known as insulin-dependent diabetic mellitus, or IDDM) and multiples sclerosis can be treated with anti-human CD3 antibody. The invention’s antibodies are best used with low-dose regimens, chronic regimens, or regimens involving redosing following a period of time. The invention provides for the administration of antibodies which bind specifically to the epsilon-subunit of the human CD3 complex. These antibodies regulate the interaction between the T-cell receptor and the alloantigen, and thus the T-cell mediated cytotoxicity that is associated with autoimmune diseases. The invention also provides for the use of modified anti-human CD3 antibody that exhibits reduced or eliminated T cell activation and effector function as compared with non-modified antibodies.

Background for Methods of treating autoimmune diseases using monoclonal immunosuppressive antibodies with reduced toxicities
2.1 Autoimmune Diseases
Autoimmune disease is caused when the immune system attacks itself. Organs, tissues and cells. Autoimmunity is the mobilization of immune system against self-targets. Autoimmunity occurs in all individuals, but rigid control systems suppress self-recognizing immune cells to the extent that autoimmunity remains asymptomatic. When there is a disruption in the control system that allows the autoimmune cells escape suppression or when there are changes in a tissue target such that it no longer recognizes itself as self, disease states can occur. These changes are caused by aberrant immune stimulation, which is not fully understood. However, it has been hypothesized that genetically predisposed people will experience these changes.
Autoimmune disorders can be systemic or organ-specific and are caused by different pathogenic mechanisms. Organ specific autoimmunization is characterized by tolerance and suppression within the T cell compartment, aberrant expression of major-histocompatibility complex (MHC) antigens, antigenic mimicry and allelic variations in MHC genes. Systemic autoimmune disorders are characterized by polyclonal activation of B cells and abnormalities in immunoregulatory immune T cells, T-cell receptors, and MHC genes. Diabetes, cutaneous Psoriasis (psoriasis of the skin), ulcerative colitis (ulcerative colitis), hyperthyroidism (autoimmune adrenal insufficiency), hemolytic anemia and multiple sclerosis are examples of organ-specific autoimmune diseases. Systemic autoimmune disease examples include systemic Lupus, Erythematosus, Rheumatoid Arthritis, Psoriatic Arthritis, Sjogren Syndrome Polymyositis, Dermatomyositis, and Scleroderma.
Organ transplant recipients, even though they do not have an autoimmune disease, often suffer from similar symptoms to those of autoimmune patients and need similar treatments. The immune system attacking the transplanted organs can cause organ failure or other systemic complications.
There is an urgent need for better strategies to modulate the immune response and/or treat autoimmune diseases.” Immune system disorders are currently treated with immunosuppressive drugs such as cortisone and derivatives of aspirin, hydroxychloroquine and methotrexate. Other agents include azathioprine and cyclophsophamide, as well as various biologics like anti TNF antibodies. Treatments are successful in varying degrees, depending on the patient and disorder. The use of general immunosuppressive therapy can be a problem because the higher the level of immune-suppression and the greater the potential for success in treating the autoimmune disorders, the greater the risk of opportunistic infection. Due to the compromised immune system of the patient, even minor infections can quickly become a serious concern.
2.1.1 Diabetes
Diabetes is usually classified into two types, type 1 and type 2. Type 2 diabetes, a non-autoimmune condition, is usually diagnosed in adults. The disease is progressive and occurs when the body fails to produce enough insulin, or does not use it efficiently (this is known as insulin resistant). Type 2 diabetics are usually over 45 years old, overweight or obese (BMI 25 or greater) and physically inactive. They also have high blood pressure (140/90 mmHg in adults) and low HDL cholesterol (35 mg/dL).
Type 1 diabetes (also known as juvenile diabetes, insulin-dependent diabetic mellitus or adult-onset type 1 diabetes) is an autoimmune disorder that is usually diagnosed in children. In the United States, IDDM affects approximately 15 million people. An estimated 12 million of these people are asymptomatic and unaware they have this condition. Type 1 diabetes is associated with presumptive genes, childhood viruses, other environmental factors and/or other autoimmune disorders. The genetic factors that are associated with type I diabetes are still not completely understood. However, the risks of developing the disease can be linked to family history and ethnicity. A child with a parent with type 1 diabetic is at a greater risk than a sibling or child without diabetes. The genetic factors that are linked with type 1 diabetes risk appear to be linked with an HLA type. For example, HLA DR3 and DR4 is associated with higher risks in Caucasians. HLA DR7 is also associated with higher risks in African descent people.
Unknown factors such as childhood viruses, or exposure to other environmental factors (e.g. exposure to certain food or chemicals) are also thought to activate or potentiate an inherited gene and cause type 1 diabetes. Coxsackie B, enteroviruses and adenoviruses have all been linked to type 1 diabetes. Rubella, cytomegaloviruses and Epstein Barr virus are also viruses that may be associated. The presence of other autoimmune diseases, such as celiac and thyroid disease, increases the risk of type 1 diabetes.
Type 1 Diabetes is caused primarily by an autoimmune reaction in which the insulin-producing?-cells (also called islet cells) of the pancreas are slowly destroyed. Insulitis is the early stage of diabetes, characterized by the infiltration of leukocytes in the pancreas. It is also associated with pancreatic inflammation as well as the release of anti?-cell cytotoxic antibody. As the disease advances, the damaged tissue may attract lymphocytes causing further damage to?-cells. A general activation in lymphocytes in response to viral infections, food allergies, chemicals, or stress may also result in the destruction of more islet cells. The early stages of diabetes are often missed or misdiagnosed, as the clinical symptoms usually appear only after 80% of?-cells has been destroyed. Type-1 diabetics are insulin-dependent for the rest of their lives once symptoms appear. Diabetes is associated with a dysregulation of blood glucose levels that can cause blindness, kidney damage, nerve damage, and stroke.

2.1.2 Multiple Sclerosis
Multiple sclerosis is an inflammatory, chronic and often debilitating disease of the central nerve system. Multiple inflammatory foci are characterized by gliosis and axonal damage in the brain and spine cord. The cause of the disease, however, is unknown. However, a convergence of evidence suggests that it’s caused by an immune dysfunction. This disruption allows cells of the immune to attack the myelin sheath, which surrounds axons in the CNS, i.e. the brain and the spinal cord. Plaques consist of inflammatory and astroglial cell, edema and fragments of myelin. Electrical impulses can’t travel along the nerve fiber pathways of the brain or spinal cord quickly when myelin has been damaged. Electrical conductivity disruption can cause fatigue, as well as disturbances in vision, strength and coordination, balance, bladder and bowel functions, and sensations. The symptoms can include: weakness, paralysis, tremor, muscle atrophy, abnormal movement, numbness, tingling or abnormal sensations in any part of the body, pain in extremities or facial areas, double vision, discomfort in the eyes, uncontrollable rapid movements of the eye, decreased coordination, balance loss, decreased ability of small or intricate movements to be controlled, abnormal gait, muscle spasms or spasms in general, dizziness, vertigo and decreased ability to control movements. The symptoms are recurring, lasting from days to months. They then diminish or disappear. The symptoms can change or even be different with each recurrence as the affected areas may have changed.
Studies of the natural history suggest that there are various patterns of disease activity. Some patients experience rare attacks while others have frequent attacks. Others gradually and steadily worsen, without any attacks. The benign MS is a condition in which patients have few attacks but are still minimally disabled 10 years after diagnosis. This group represents only 10-15% of all MS patients, but there are some indications that it may be more prevalent than currently thought. Relapsing-remitting MS is defined as a condition in which patients have episodes with a partial or full recovery, but are otherwise stable. About 80-90% initially have a relapsing course. About 50% of these patients will experience difficulty walking within 15 years and the remaining 80% (after approximately 25 years) will eventually develop a progressive disability, with or without attacks. Secondary progressive MS is a condition in which patients who initially experience exacerbations, but later develop gradual disability, have experienced an initial attack. About 10-15% of MS sufferers do not have an initial attack. Patients with primary progressive sclerosis will gradually worsen following the onset of their first symptoms. Some patients may experience an exacerbation. These patients have progressive-relapsing MS.
2.2 T cell Functionality in Diabetes, Autoimmune Diseases and Other Autoimmune Conditions
Destruction?-cells, myelin, and other target cells in autoimmune diseases is believed to be mediated largely by cytotoxic lymphocytes (CTLs, also known as CD8+T cells), which recognize antigenic peptides derived from target cells. CTLs and other types of T-cells recognize these antigenic, peptides via their T cell receptors (TcR). The TcR interacts with small antigens that are only present in complex with MHC proteins.
Most cells in the body have MHC molecules on their surfaces. Depending on the type of MHC, they will either present soluble antigens or those that are dispersed throughout the lymphatic and/or circulation systems. Or fragments of cytoplasmic protein. MHC molecules, also known as human leukocyte antibodies or HLA, and TcRs, are highly polymorphic. Each clonal variant recognizes and binds to a unique peptidic sequence or set of peptidic analogues. Cells that are specific to the immune systems, such as B cells and T cells, also express multiple variants of MHC molecules. Cells in the body, including B and T cells express different variants of MHC, with each variant binding a specific peptide. During maturation, T and B cells, respectively, lose their ability to express different variants of MHC. Mature T-cells will, therefore, express only one variant of TcR, and will recognize/bind to a single MHC/antigen.
The binding of a TcR with a MHC/antigen leads to an intracellular signaling cascade, called activation, within the T-cell, which leads to clonal proliferating of the cell and specific class-specific responses. For example, in CTLs the response to activation also includes the release of cytotoxic enzymes that result in apoptosis/destruction of the target cell.
2.3 Modulation by Monoclonal Antibodies of T-Cell Activation
The discovery that at least some autoimmune diseases can be attributed to aberrant T-cell action led to the development of therapeutics that eliminate problematic T-cell clones that express TcRs that are directed against self antigens or reduce unwanted T cell activation/activity. T cell activation by TcR-binding is a complex phenomenon, due to the involvement of many cell surface molecules on the responding T cells (Billadeau and al., J. Clin. Invest. 109:161-168; Weiss, 1990, J. Clin. Invest. 86:1015-1022; Leo et al., 1987, PNAS 84:1374-1378; Weiss et al., 1984, PNAS 81:4169-4173; Hoffman et al., 1985, J. Immunol. 135:5-8).
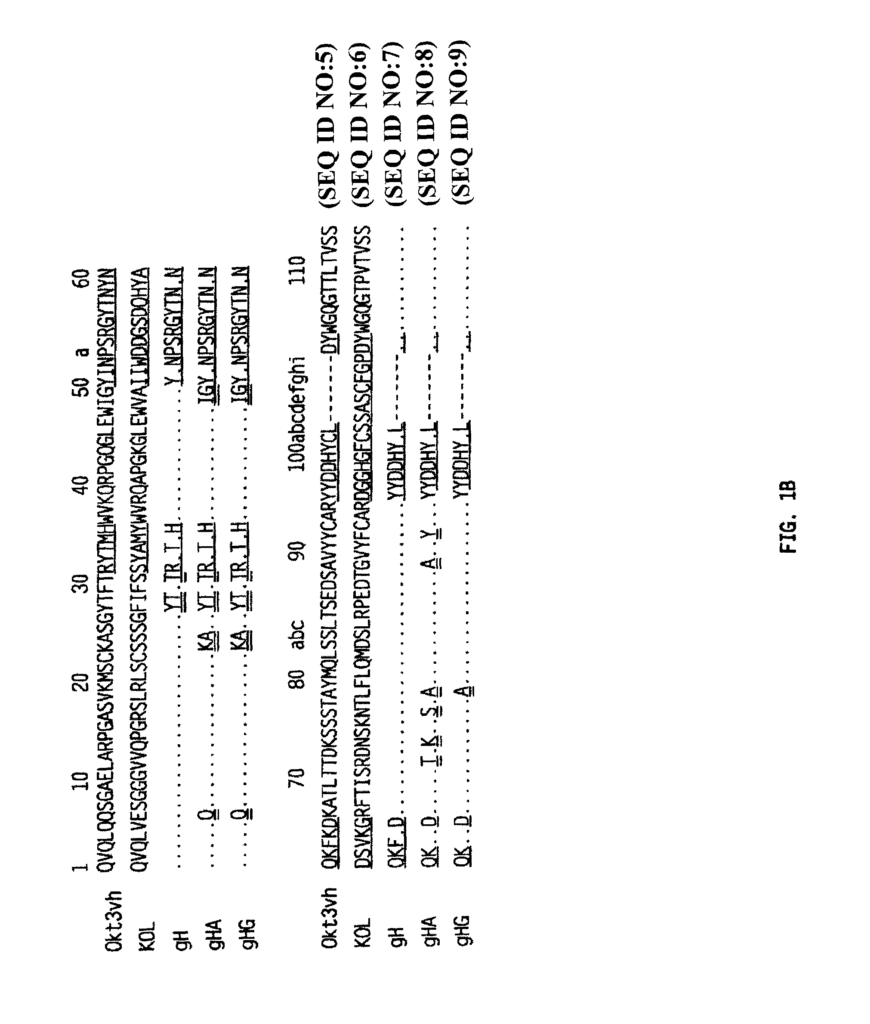
Targeted therapy directed against general T-cell activation was problematic because the TcR is composed by a disulfide linked heterodimer containing two integral membrane glycoprotein chains that are clonally spread, “Targeted therapies directed against general T cell activation were problematic in that the TcR is composed of a disulfide-linked heterodimer, containing two clonally distributed, integral membrane glycoprotein chains. The most common research on modulation of T cell activation was done in connection with improving immune suppression in organ transplant recipients. The majority of research on modulating T cell activation has been done to improve immune suppression among organ transplant recipients. Monoclonal antibody therapy was one of the first methods to reduce T cell activation selectively. U.S. Pat. No. No. CRL-8001, which produces a monoclonal murine antibody against an antigen that is found on virtually all normal human peripheral cells. Binding OKT3 to human T cells in vivo causes a pronounced and reversible immune suppression. OKT3 recognized an epitope within the CD3 complex of the human 8-subunit (Salmeron and al., 1991). 147:3047-3052; Transy et al., 1989, Eur. J. Immunol. J. Immunol. No. 4,658,019). The CD3 complex, also known as T3, is composed of low-molecular-weight invariant proteins that noncovalently bind to the TcR. (Samelson, et. al., 1985 Cell 43:223-231). CD3 structures may represent accessory molecules which could be used to transmit activation signals triggered by the binding of TcR. The CD3 structures are thought to represent accessory molecules that may be the transducing elements of activation signals initiated upon binding of the TcR?-?
![]()
