Invented by Wing Cheung, David Gibson, Christine Cote, Els Vercammen, Janssen Pharmaceuticals Inc
The Janssen Pharmaceuticals Inc invention works as follows
The present invention relates to systems and methods for obtaining optimized EPO dosage regimens for a desired pharmacodynamic/pharmacokinetic response. The system includes choosing one or more EPO dosage regimens, then using a PK/PD model to determine the pharmacodynamic/pharmacokinetic profile of one or more EPO dosage regimens, and finally selecting one of the EPO dosage regimens for administration to achieve the desired pharmacodynamic/pharmacodynamic response based on the EPO profile.

Background for Pharmacokinetics and pharmacodynamic modelling of erythropoietin Administration
Erythropoietin is responsible for regulating red blood cells production in steady-state conditions, and for speeding up the recovery of red cell mass after hemorrhage. EPO is a glycoprotein with a 30 KDa molecular weight. It is highly glycosylated to prevent rapid degradation of the EPO molecules in vivo. Human serum EPO concentrations range between 6 and 32 U/l. The half-life of EPO (t1/2) is 2 to 13 hours, with a distribution volume close to plasma. Less than 10% of the EPO excreted by urine is expected, as it is a sialoglycoprotein. Clin. Lab Haem. 18:137-145.)
The primary site of EPO synthesis is in the kidney. Although the liver and the bone marrow are also implicated, data remain inconclusive. Hypoxia in tissues is the primary cause of increased EPO production. Hypoxia may be caused by large blood losses, radiation-induced destruction of red cells, or high altitude exposure. Hypoxia can also be caused by anemia, since red blood cell transport is responsible for oxygen in the body. In the normal state an increase in EPO stimulates production of red blood cells, thereby increasing the oxygen level and reducing or eliminating hypoxia.
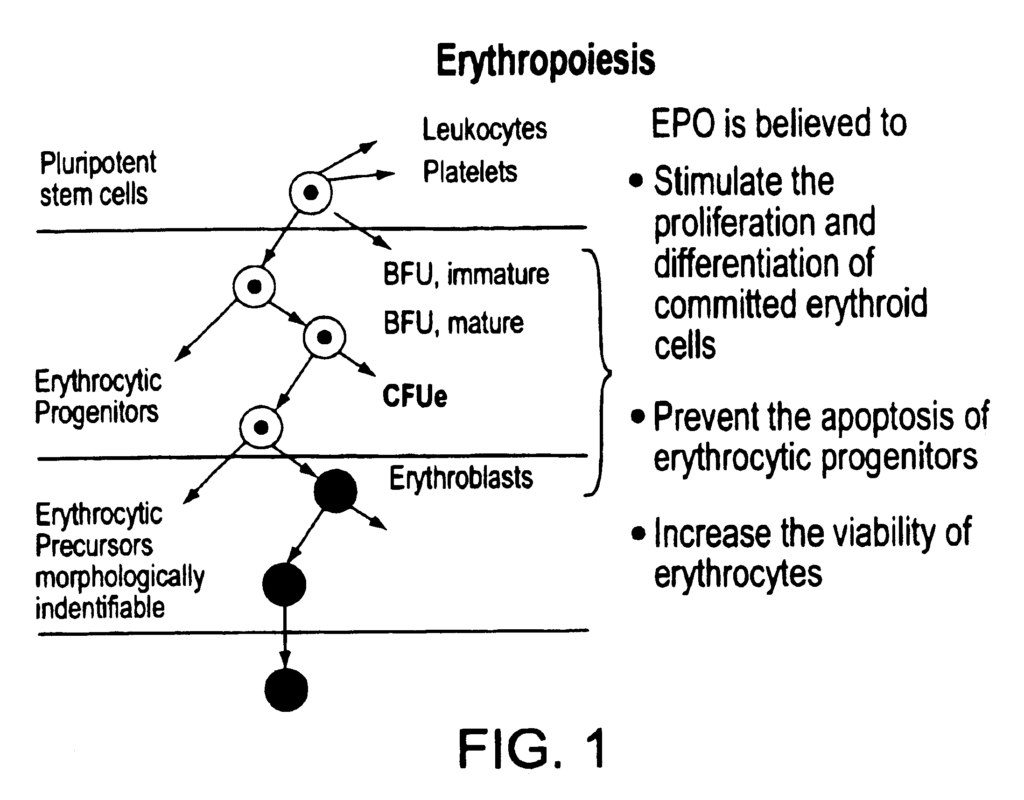
The principal function of EPO, in conjunction with other growth-factors, is to stimulate proliferation and differentiation of the erythrocytic precursor cells in the bonemarrow. This leads to reticulocytosis in the bone marrow and an increase in RBCs in the blood. 1). Cell differentiation along the lineage of erythroid cells occurs in humans over a period of two weeks. The BFU-E is the earliest progenitor. It is small, and has no distinguishing histologic features. CFU-E, which is larger than BFU and precedes hemoglobin formation, is the next stage after BFU. Immature erythrocytes are the cells that start producing hemoglobin. They also begin condensing nuclei, eventually becoming mature erythroblasts. The mature erythroblasts have a smaller nucleus than immature cells and a more compacted one. This is subsequently expelled when the cells are transformed into reticulocytes. The reticulocytes were named this way because they contain reticular polyribosome networks. As the reticulocytes shed their polyribosomes they mature into mature red blood cells.
Until recently, EPO was very hard to come by. The protein is found in urine but the excreted levels of EPO are too low for this to be a useful source. Identification, cloning and expression of genes that encode EPO, and techniques for EPO purification, such as those described in U.S. Pat. Nos. EPO is now readily available to be used in therapeutic applications. U.S. Pat. includes a description of how to purify recombinant EPO from the cell medium used to grow mammalian plasmids containing recombinant EPO. No. 4,667,016. The amino acid sequence of this recombinant EPO is identical to the human urinary erythropoietin. They are virtually indistinguishable by chemical, physical, and immunological tests. Recombinant EPO that is biologically active has been produced from mammalian cells containing the EPO genes on recombinant DNA plasmids. This EPO can be used for therapeutic purposes. The knowledge of the sequence of the gene and the availability in larger quantities of purified proteins has also led to an improved understanding of its mode of action.
The biological activity of a molecule is determined by its structure. The primary structure, or amino acid sequence of a particular protein, is what allows a polypeptide to form secondary structures (e.g.?-helix, or?pleated sheet), and tertiary structures (overall three-dimensional folding) during and after its synthesis. The biological activity of a polypeptide is governed not only by its structure but also by the modifications that are generated after it has been translated. In fact, many secretory and cell surface proteins are modified with one or more oligosacchride group. This modification, known as glycosylation can have a dramatic effect on the physical properties and function of proteins. It can also be crucial for protein stability, secretion and subcellular location. “Proper glycosylation is essential for biological activity.
Both human urinary-derived EPO and recombinant human EPO (expressed by mammalian cell) have three N-linked chains and one O linked chain, which together make up about 40% of total glycoprotein molecular mass. It has been demonstrated that the oligosacchride chain is modified with sialic acids at their terminals. The in vitro activity of glycosylated EPO is affected by enzymatic treatment to remove all residues of sialic acids. Chem. 249:4202). This behavior can be explained by the rapid clearance of asialoerythropoeitin (H. asialoglycoprotein-binding protein) from the blood circulation after interaction with this protein. Chem. 243:155; Briggs et al., 1974, Am. J. Physiol. J. Physiol. 50:287). EPO is biologically active in vivo only when sialylated, to avoid binding with the hepatic protein binding protein.
Anemia is often associated with a deficient or inefficient EPO production. Anemias of chronic diseases (chronic infections, rheumatoid, and autoimmune disease) and cancer are among them. These conditions have been linked to the production of a factor which has been shown as an inhibitor of EPO. “Aplastic anemia and iron deficiency, megaloblastic and pure red cell anemias as well as myelodysplastic and thalassemias are all EPO-independent anemias.
The measurement of EPO in serum is clinically important. The determination of EPO in serum can help distinguish between anemias or polycythemias associated with increased EPO and those not. A low serum EPO level is also a requirement for concluding an anemic person may benefit from exogenous EPO.
In clinical trials, Epoetin Alpha has been tested on normal patients and patients with anemic conditions. Epoetinalfa produces a rapid haematological reaction in healthy human volunteers, if sufficient iron is available to support the increased hemoglobin synthesis. Most trials investigated the effectiveness and safety of Epoetin alfa in treating anemia that is associated with kidney failure. Epoetin-alfa can also be used to treat anemia caused by other medications, such as cisplatin, zidovudine, or platinum-based chemotherapy. Epoetin-alfa therapy has many potential therapeutic applications. For example, Epoetin-alfa treatment increases the ability of autologous blood donors to donate blood to patients who are scheduled for surgery. It also reduces the hemocrit drop that is often seen with untreated autologous donor.
Another application of EPO for improving the performance of athletes is to cause an increase in their hematocrit. This increase in hematocrit allows more oxygen to be transported from the lungs into the working skeletal muscles. Since bioengineering has made it possible to synthesize EPO, the practice of injecting blood into athletes, or what is known as EPO doping, became popular. Rev. Med. Liege 53(8): 499-502).


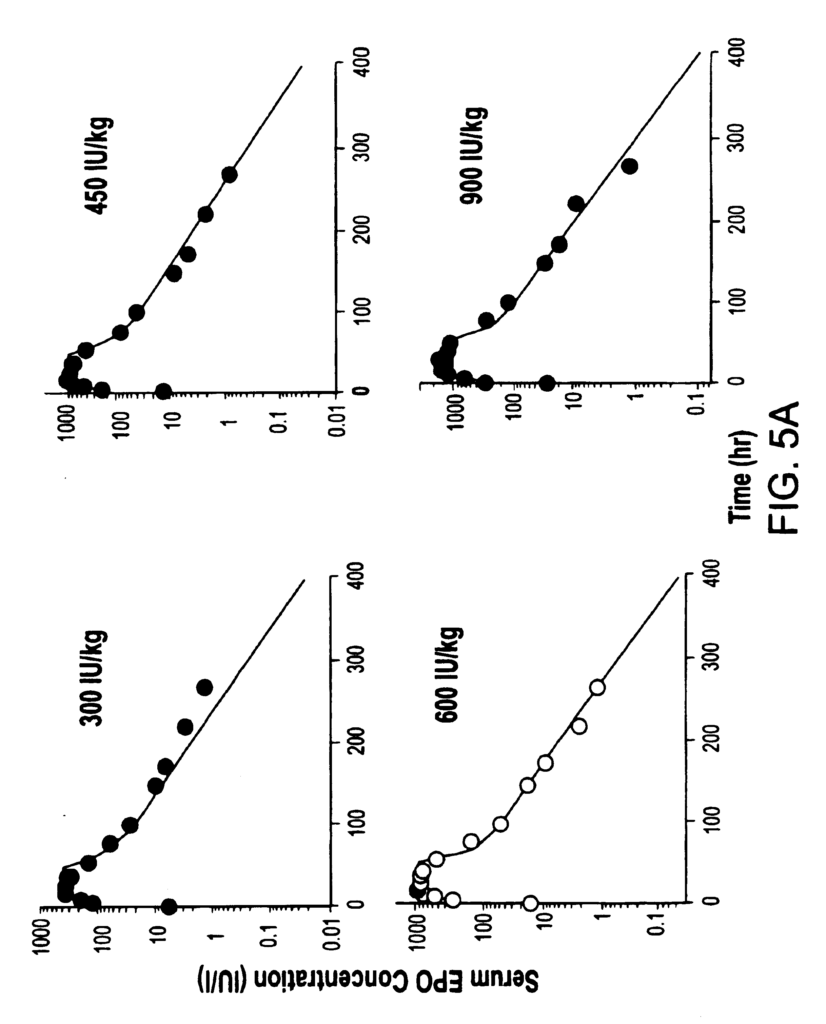
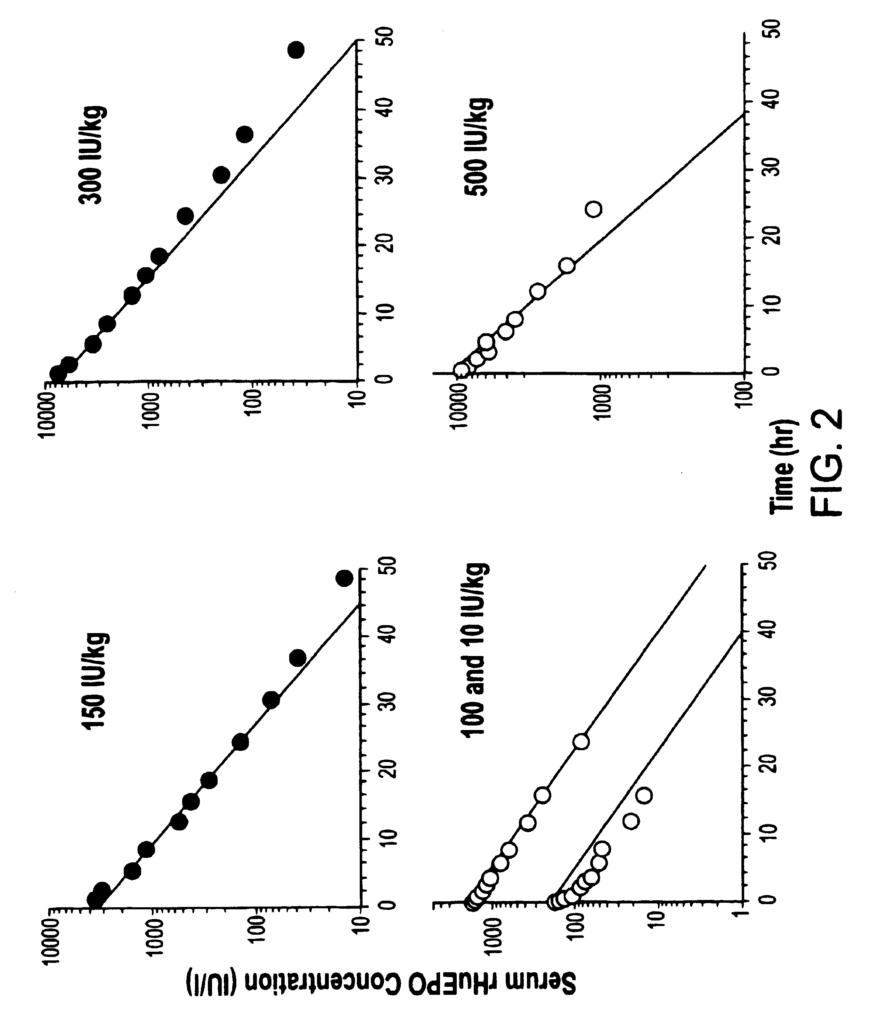
At present, the standard EPO dose regimen is associated with a number disadvantages. For specific indications such as cancer, the subjects are given 150 IU/kg EPO three time per week. It is therefore important to switch from the current approved dosing regimen to one that is more convenient. A less frequent administration is expected to improve the user’s convenience and acceptance. Standard dosing regimes may also not maximize the physiological response of the patient, and may not be cost-effective.
The rapid delivery of rHuEPO by intravenous means a lower bioavailability for longer periods of time and may not be effective in stimulating the production of RBC.
For all the reasons listed above, it is necessary to find a more effective way of administering EPO and a dosage regimen that works.
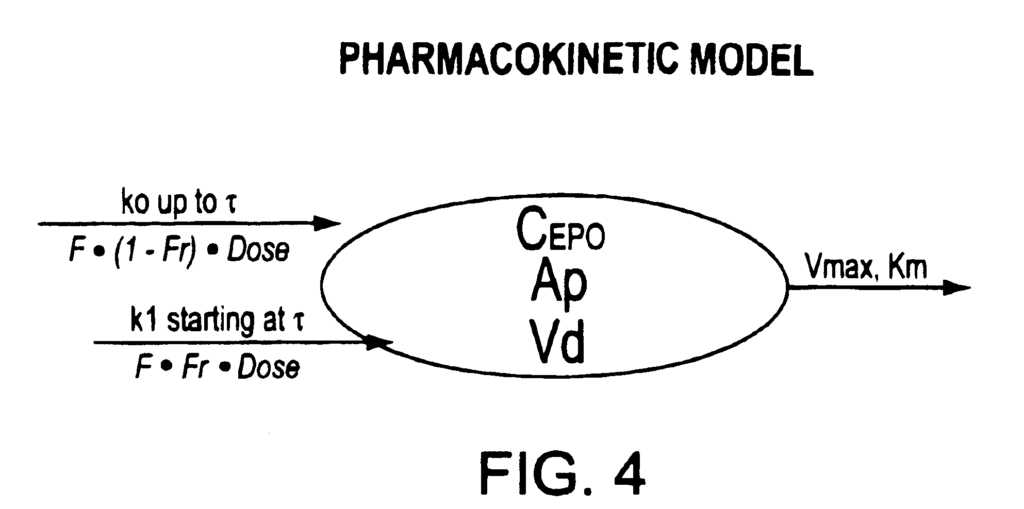
Therefore, one aspect of the present invention is the development of a pharmacokinetic/pharmacodynamic (PK/PD) model for characterizing and predicting responses to rHuEPO thereby identifying the most efficient, cost effective, and/or convenient treatment regimens for patients. In one embodiment, EPO is administered once a week or twice a month. A further aspect of the invention is a method for evaluating the pharmacokinetics and pharmacodynamics of EPO following administration of two or multiple dosing regimes to compare clinical outcomes, tolerance and safety parameters. Also contemplated are associated business methods and computer system.
A specific embodiment of the invention can include a method of obtaining optimized EPO dose regimens to achieve a desired pharmacodynamic reaction. This can involve selecting one or more EPO regimens and then using a model PK/PD to determine the pharmacodynamic profiles of one or multiple EPO regimens. Finally, one of the EPO regimens is selected for administration in order to achieve the desired (PD) response according to the EPO profile. In an alternative embodiment, PD response may include one or more from the group consisting reticulocyte count, RBC level, and hemoglobin levels.
The present invention can also take the form of a method of determining optimal EPO dose regimens to obtain a desired pharmacodynamic reaction. This involves selecting desired pharmacodynamic reactions, using a PK/PD to determine an EPO regimen that will provide the desired response, and then selecting the EPO regimen to be administered to achieve the desired response. In another embodiment, the PD can be one or more from the group consisting reticulocyte count, RBC level, and hemoglobin levels.
Another preferred embodiment of the invention can include an computer program that can be used to obtain optimized dosage regimens in order to achieve a desired response pharmacodynamically. The computer program can be a computer code. In another embodiment, the code allows the user select one or several desired pharmacodynamic effects. The computer code uses the PK/PD to determine EPO dose regimens that will provide the desired pharmacodynamic response. EPO can be administered either weekly or every two weeks depending on the body mass. The weekly EPO dosage may include administering EPO with a dose of 40,000 IU, and the EPO dosing regime once every two week may include administration of EPO with a dose of approximately 80,000 to 120,000 IU. In an alternative embodiment, the PD can be comprised of one or more from the group consisting reticulocyte count, RBC level, and hemoglobin levels.
An alternative preferred embodiment of the invention may include an computer program for obtaining optimal dosage regimens to achieve a desired response in terms of pharmacodynamics.” In a further embodiment, the program is a computer code. The computer code can allow the user select one or several EPO dosage regimens. The computer code uses the PK/PD to calculate a pharmacodynamic reaction based on EPO dosage regimens.
In a preferred embodiment, the computer program may be used to determine optimized EPO dose regimens for a desired response. This includes selecting one or more EPO regimens and using a PK/PD model for determining the pharmacokinetic responses of these regimens. Then, the selected EPO regimen is selected based on the pharmacokinetic profile. In a further embodiment, pharmacokinetic responses may include serum levels of EPO, bioavailability and EPO thresholds.
A further embodiment of the invention can include a method of obtaining optimized EPO dose regimens for a desired response pharmacokinetic. This may involve selecting one or several desired responses pharmacokinetic, using a PK/PD to determine an EPO dose regimen that will provide one or more of these desired responses pharmacokinetic, and then selecting the EPO dose regimen that gives the desired responses pharmacokinetic.

A computer program that includes a code describing a PK/PD EPO model can be used to obtain optimized EPO dose regimens. In another embodiment, the computer program may allow the user select one or multiple pharmacokinetic response, and then use a PK/PD to determine EPO dosage regimens which provide the desired pharmacokinetic response.