Invented by Robert F. Nease, JR., Katherine Harini Sundararaman, Heather D. Sundar, Krista Lynn Theby, Tina Lynn Bauman Butcher, Express Scripts Strategic Development Inc
Member messaging refers to the process of communicating with members of an organization or community. This can include sending out newsletters, updates, and announcements, as well as responding to inquiries and feedback. Effective member messaging is crucial for building strong relationships with members and keeping them engaged and informed.
There are several methods for member messaging available in the market today. One of the most popular methods is email marketing. Email marketing allows organizations to send out newsletters and updates directly to members’ inboxes. This method is cost-effective and can be easily automated, making it a popular choice for businesses of all sizes.
Another popular method for member messaging is social media. Social media platforms like Facebook, Twitter, and Instagram provide businesses with a direct line of communication to their members. This method is particularly effective for reaching younger audiences who are more likely to be active on social media.
Messaging apps like WhatsApp and Telegram are also becoming increasingly popular for member messaging. These apps allow businesses to send out personalized messages directly to members’ phones. This method is particularly effective for urgent updates and time-sensitive information.
In addition to these methods, there are also specialized platforms for member messaging. These platforms provide businesses with a range of tools for managing and automating member messaging. They often include features like segmentation, automation, and analytics, making it easier for businesses to target their messaging and track its effectiveness.
The market for methods for member messaging is expected to continue growing in the coming years. As more businesses recognize the importance of effective member messaging, they will be looking for new and innovative ways to connect with their members. This presents a great opportunity for businesses that specialize in member messaging to grow and expand their offerings.
In conclusion, member messaging is an essential part of building strong relationships with members and keeping them engaged and informed. There are several methods for member messaging available in the market today, including email marketing, social media, messaging apps, and specialized platforms. As the market for member messaging continues to grow, businesses that specialize in this area will have a great opportunity to expand their offerings and meet the needs of their clients.
The Express Scripts Strategic Development Inc invention works as follows
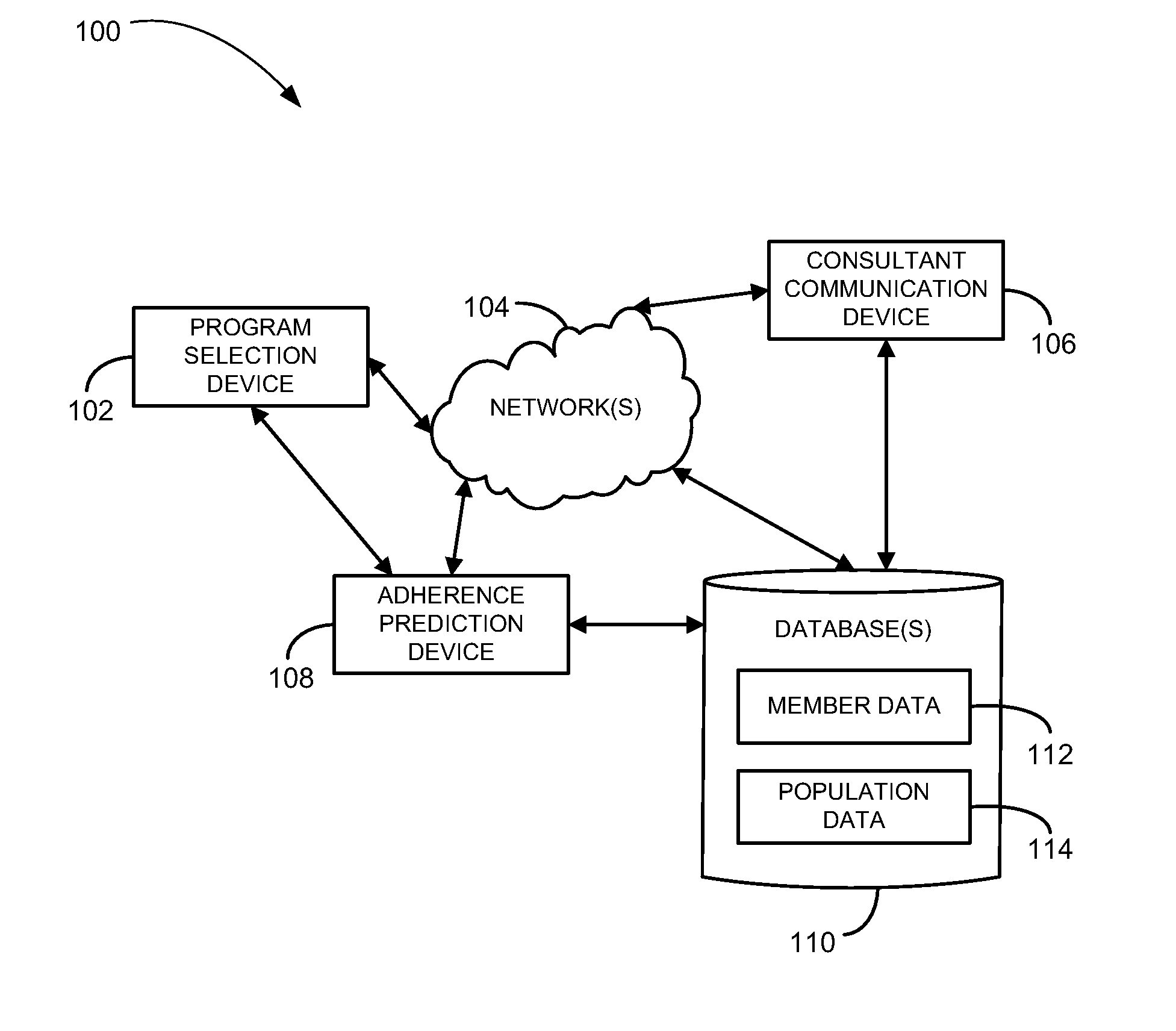
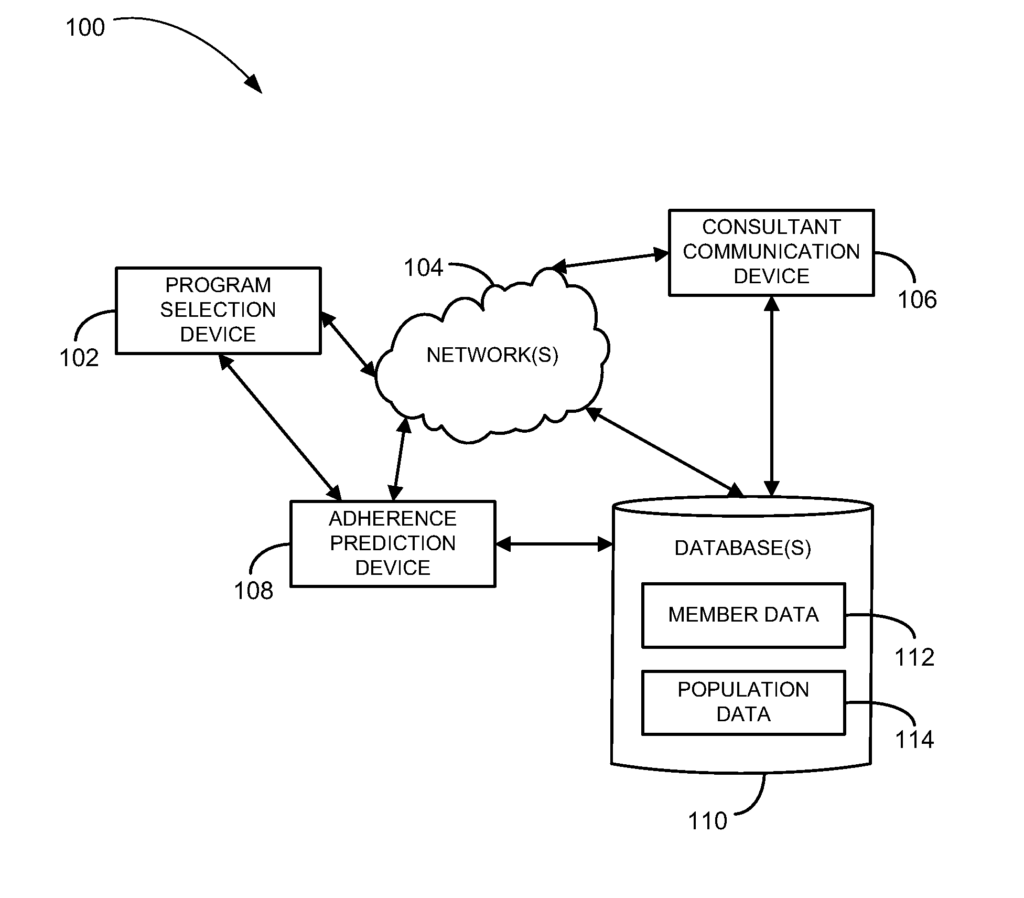
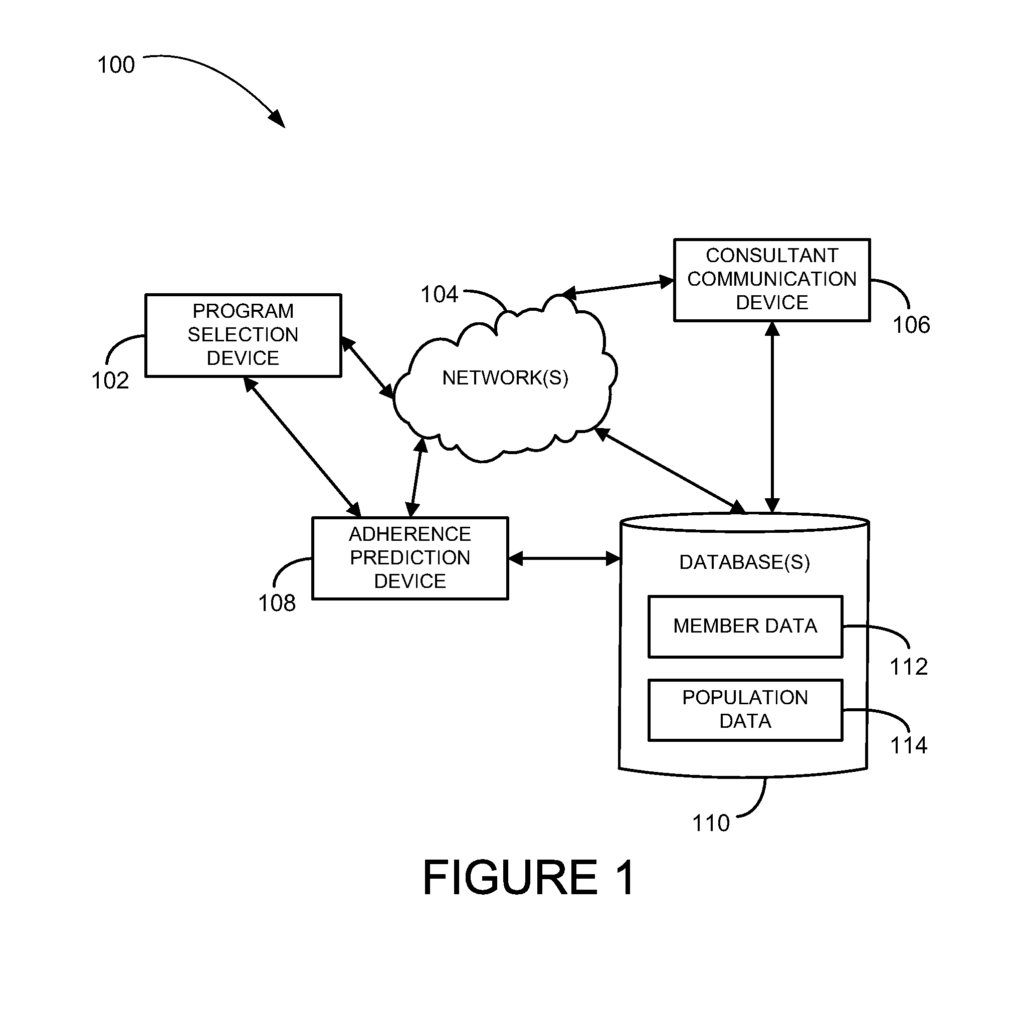
Systems and methods for improving therapy compliance are described.” In one embodiment, the disease state of a member can be identified. The member classification is determined. The member classification can be based upon past treatment the member has received for a condition that is associated with the disease. The disease state and member classification are used to select a diagnostic loop. The diagnostic loop can include multiple operations. At least one operation of the diagnostic loop’s plurality is performed. “Other methods and systems will be described.
Background for Methods for Member Messaging
Reducing the cost of health care is a constant challenge. Prescription drug coverage is one of the largest drivers of these costs. An increase in prescription drug adherence may lead to a reduction of medical costs and productivity. Non-adherence to prescription drugs can have a significant impact on an individual’s well-being, as well as the health system at large, resulting in costs of up to $100 billion per year.
Examples of methods and systems to improve therapy adherence are discussed.” For the purpose of explaining, many specific details are provided in the following description to give a complete understanding of example embodiments. “It will be obvious to anyone of ordinary skill that embodiments of this invention can be practiced even without these specifics.
The methods and systems aim to improve adherence to treatment programs, and in particular to medication therapy or healthcare therapy which includes medication therapy. These methods and systems can also be used to increase member compliance and/or adherence to other health and wellness programs.
Members may be employees or associated with an employee group, and they receive a medical benefit and/or prescription drug benefits through the health plan and/or prescription drug plan of the employer group. A company, corporation or other similar entity may be an employer group. However, it does not have clinical capabilities to provide healthcare services for its employees. Members can be employees of an employer group. Members are people who participate in a health insurance plan. Members may also be called patients.
In general, a client will engage a pharmacy benefits manager (PBM), to provide a drug benefit plan. Clients include government organizations (e.g. Federal government agencies and Departments of Defense and State Government Agencies), middle-market companies, large employers and health insurance companies who have created a drug benefit. PBMs can be standalone PBMs or part of larger organizations that offer other services or benefits. The methods and system can be used in general to direct a client who is a part of a drug benefit program to pharmacies that are associated with a network or association of pharmacy networks. The terms pharmacy networks and pharmacies network associations are used interchangeably here.
The tool for improving therapy adherence may use predictive modeling in conjunction with historical data (e.g. refill gap data) of a member to prioritize member outreach. A non-adherence score can be calculated using a combination demographic data, medical history, and other factors. Members who are identified as being at high risk for non-adherence will receive a more rapid outreach or intervention than those with a lower risk. In some embodiments the outreach or the intervention could consist of a call to the member that is a result of a tailored intervention on the basis the non-adherence index.
The methods and system described in this document may reduce unnecessary costs and member disruption as only those members who are considered to be at a high risk of failing to self-correct will receive an outreach. The interventions can be tailored to increase their effectiveness. Predicting which members will be at high risk can help to address adherence issues proactively, rather than reactively.
The methods and systems can include methods for identifying members at risk for non-adherence or non-compliance with a treatment program, predicting the basis for this non-compliance as well as targeting interventions to those members identified to be likely to not comply, taking into account the predicted basis for noncompliance. They may also include proactive outreach methods to a member in order to intervene timely and consistently. The methods and systems can also include creating benefit plans to promote adherence to a therapy program. This includes identifying members at risk of not complying with the program and predicting the basis of such noncompliance. It may then structure the benefit plan for the member in a way that increases the likelihood of compliance, or adherence, and reduces the likelihood of discontinuing the therapy.
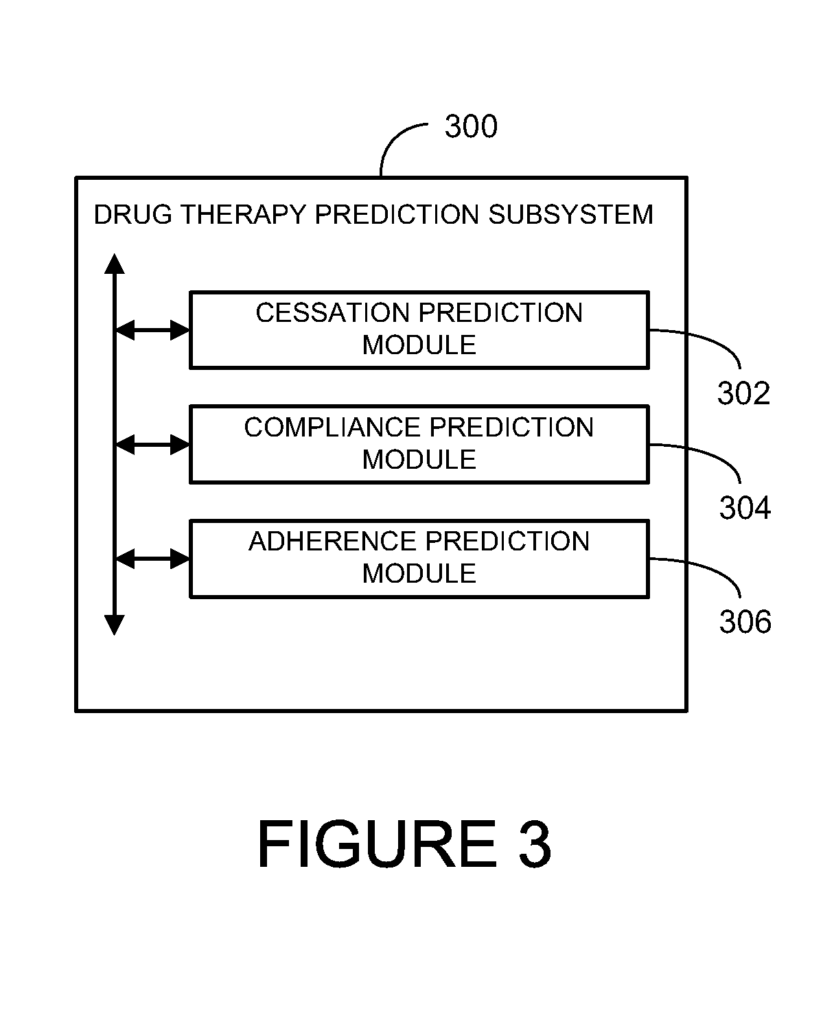
The predictive tool can be used to predict therapy compliance.
The following examples of indicators of compliance that could be related to therapy adherence are: higher income, older age, more severe disease, more medications, symptomatic diseases, being partnered, partner adherence to medication maintenance, and greater disease severity.
Other factors that may affect non-adherence include increased cost (or copayments) of medication, which can result in a decrease in their use. The reverse is also true, but to a much lesser extent. Decreased cost/copayments for medications can have a modest impact on increasing adherence.
The methods and system may also include an improvement method for therapy adherence, such as promoting home delivery (e.g. mail-order pharmacies).” The promotion of home delivery is targeted at members who are less likely than others to adhere to a treatment program.
The methods and systems can be used to create plans that encourage home delivery of medications for members who are identified as being less likely to comply with the therapy. The methods and system may determine the pharmaceutical distribution channel for a member. The pharmaceutical delivery method may be the way in which a prescription drug is delivered to a patient (e.g. home delivery, mail-order, retail fill, speciality fill, etc.). The systems and methods may also detect and assess a primary cause of non-adherence for a member who is identified as being likely to not comply. The identification of the member as being likely to not comply may be done simultaneously with the identification of the primary non-adherence causes.
A member may receive a prescription medication as part of the treatment for a specific medical condition or illness. When participating in drug treatment, a member who takes a prescription drug can be considered adherant if they take the drug exactly as prescribed. The member who does not follow the prescribed dosage or frequency (e.g. the correct times and/or the right number of times) may be considered not adherent. Methods and systems can be used to improve adherence and to reduce failures.
Interventions may be included in programs to increase adherence. Interventions may include: letters to members, home delivery, specialty pharmacies to refill prescriptions, devices to remind patients to take their medication, remind them if they have missed a dose, or remind them that a refill was due, etc.
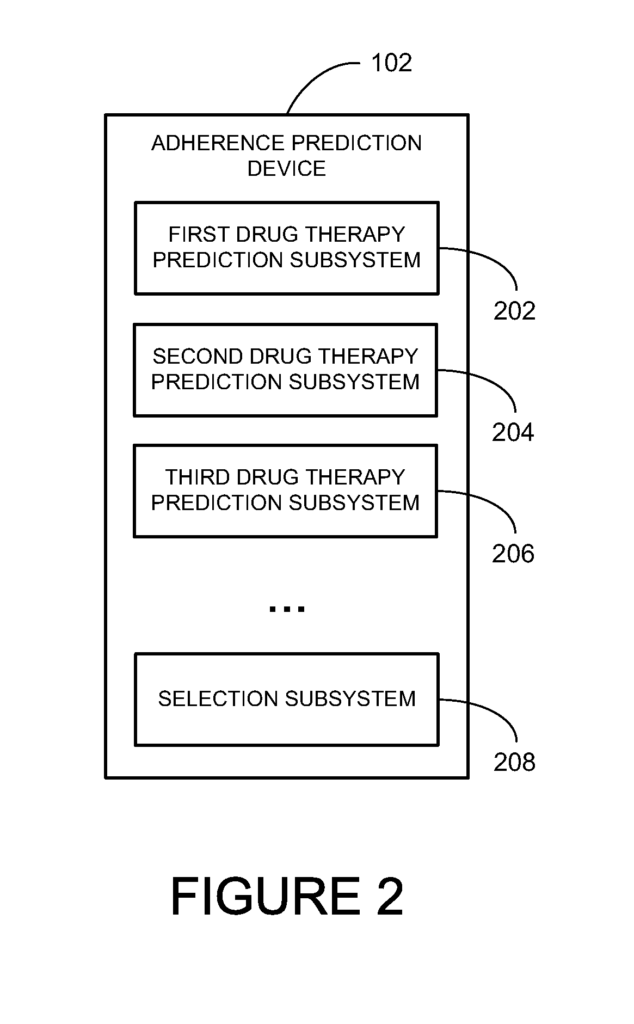
A therapy adherence proactive approach (TAPO) may be used where a consultant contacts the member by phone, email, text message or another electronic communication method. The consultant can use a consultant interface tool that runs on a computer system. The consultant can be given scripted questions that they should ask the member to diagnose the cause(s) of non-adherence. The consultant can enter the responses of the member into an interface, and then be asked additional diagnostic questions or offered alternative programs that could help the member. The computer system may initiate a logic branch that includes the scripted questions and helpful hints, as well as the program offers. The computing system may contain one or more logic trees. In the case of multiple logic trees, a member may choose one over another based on factors such as demographics, predictive markers, type and state of disease, drug therapy or other factors. In another embodiment, a large logic tree with major branches or paths may be selected using the same types of factors. In either case, sections of the logic can be bypassed based on factors related to the members.
In one embodiment, a member can be contacted by a fully automated computer-to-human communications system, a highly advanced Interactive Voice Response (IVR), utilizing a sophisticated automated attendant voice, voice/speech and/or touch-tone recognition, Dual-Tone Multi-Frequency signaling technology, or other electronic communication such as text messages, instant messaging or web content. A logic tree of possible diagnostic questions can be used to provide the intelligence of the system. Therefore, rather than utilizing a live attendant or consultant with a consultant user interface that prompts the consultant/attendant, the system may be fully automated with a fully automated attendant where the intelligence of the automated attendants questions and the responses, hints or suggestions all stem from the logic tree.
In one embodiment, a member who is potentially non-compliant may also be associated with three primary causes of non-adherence. Sporadic forgetters include members who are positive about therapy but are not intentionally avoiding it. They may occasionally forget to take their medication, and are therefore not adherent.
Active decliners might not value their therapy for a number of reasons. It could be because they believe the medication is ineffective, are experiencing side effects or don’t like to be “prescribed” for. They may not like being?prescribed for,’ or believe that the medication is ineffective. They actively decide not to take the prescribed medication.
Refill procrastinators are good at taking their medication as long as there are pills available. They delay getting a new supply as their stock runs out. They may suffer a gap in their care as a result. This is a less deliberate behavior than the active decliners, and it does not reflect an unfavorable view of therapy.
After identifying a member at risk of nonadherence or determining the primary cause of nonadherence, one embodiment of the methods can include targeting those identified members for an intervention. The intervention can take into account the primary cause of non-adherence for the member. “Interventions can include, for example, letters that combine authority (e.g. signed by a chief medical officer or physician) with loss aversion, (pointing out the risks of nonadherence instead of benefits of adherence); a reduction in copayments; reminders systems (especially effective for sporadic forgotters); auto-refill program (particularly for refill procrastinators); and financial assistance (particularly for active decliners).
Click here to view the patent on Google Patents.
Leave a Reply