Invented by Lavinia Diana Cicortas Gunnarsson, Didrik Paus, Cancer Research Technology Ltd
The market for antibodies is primarily driven by the growing prevalence of chronic diseases such as cancer, autoimmune disorders, and infectious diseases. Antibodies are widely used in the diagnosis and treatment of these diseases, making them an essential tool in the healthcare industry. The increasing demand for personalized medicine and targeted therapies has also contributed to the growth of the antibody market, as these proteins can be engineered to target specific cells or molecules in the body.
In addition to their use in healthcare, antibodies are also widely used in research and development. They are used to study the structure and function of proteins, as well as to develop new drugs and therapies. The growing demand for antibodies in research has led to the development of new technologies and platforms for antibody production, such as recombinant DNA technology and phage display.
The market for antibodies is highly competitive, with numerous companies and research institutions involved in the production and development of these proteins. Some of the key players in the market include Roche, Novartis, Amgen, and AbbVie. These companies are investing heavily in research and development to develop new and innovative antibody-based therapies and diagnostic tools.
Despite the growing demand for antibodies, there are some challenges facing the market. One of the main challenges is the high cost of antibody-based therapies, which can limit their accessibility to patients. Another challenge is the development of resistance to antibodies, which can reduce their effectiveness over time.
In conclusion, the market for antibodies is a rapidly growing and dynamic industry that plays a vital role in healthcare, research, and development. The increasing demand for personalized medicine and targeted therapies is driving the growth of the antibody market, and new technologies and platforms are being developed to meet this demand. While there are challenges facing the market, the future looks bright for the antibody industry, with continued growth and innovation expected in the coming years.
The Cancer Research Technology Ltd invention works as follows
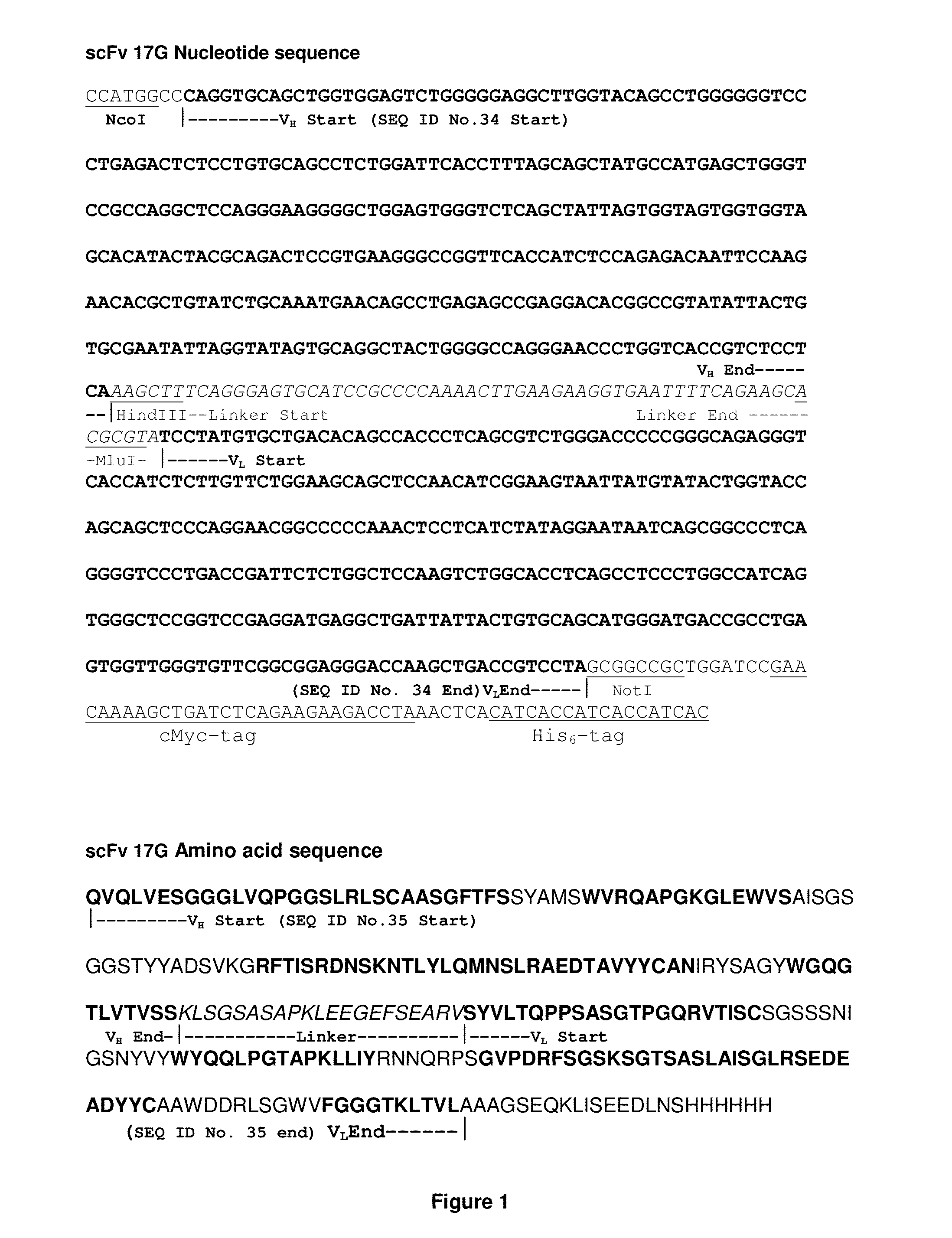
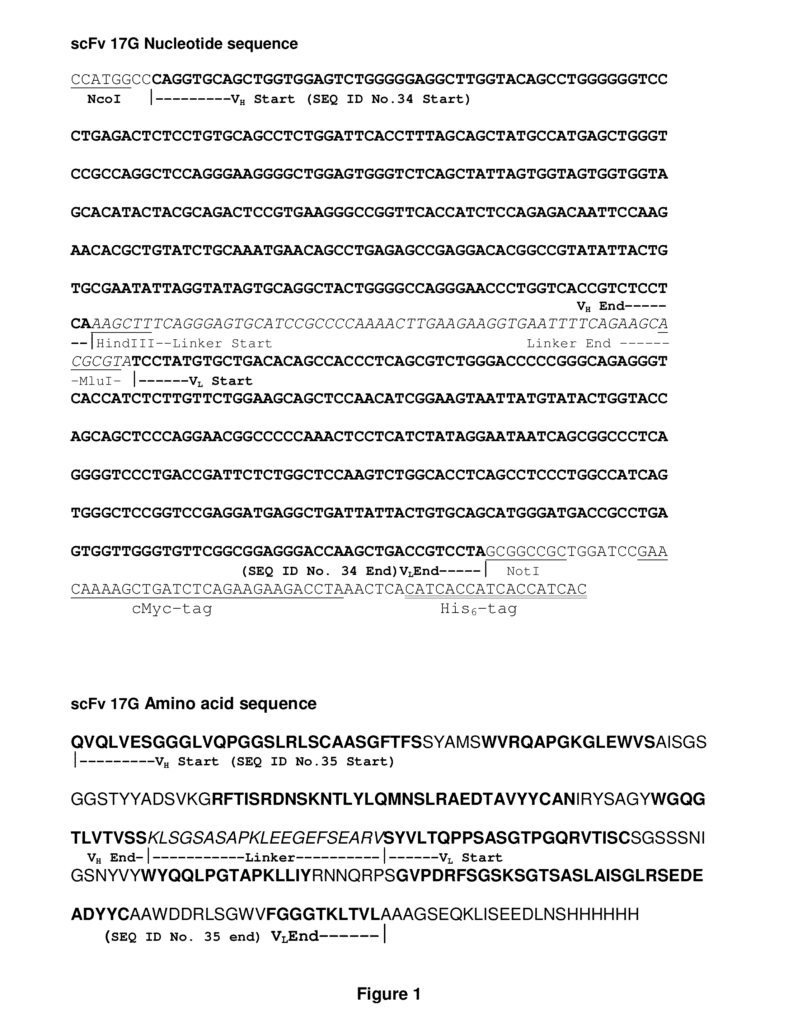
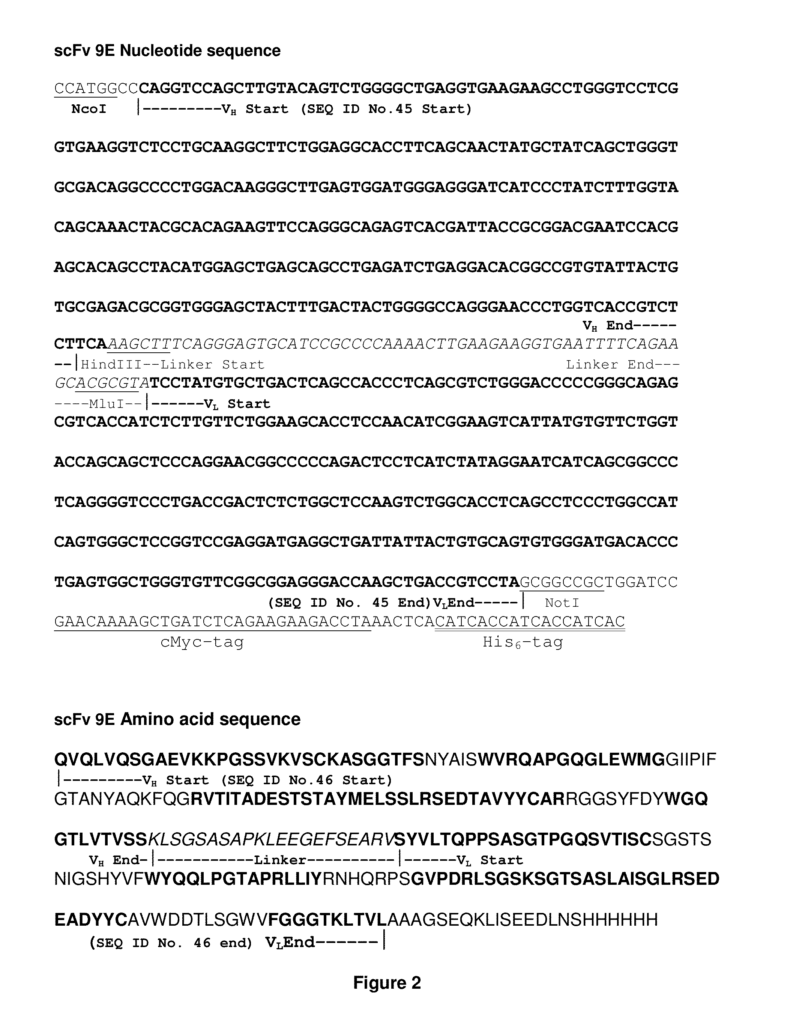
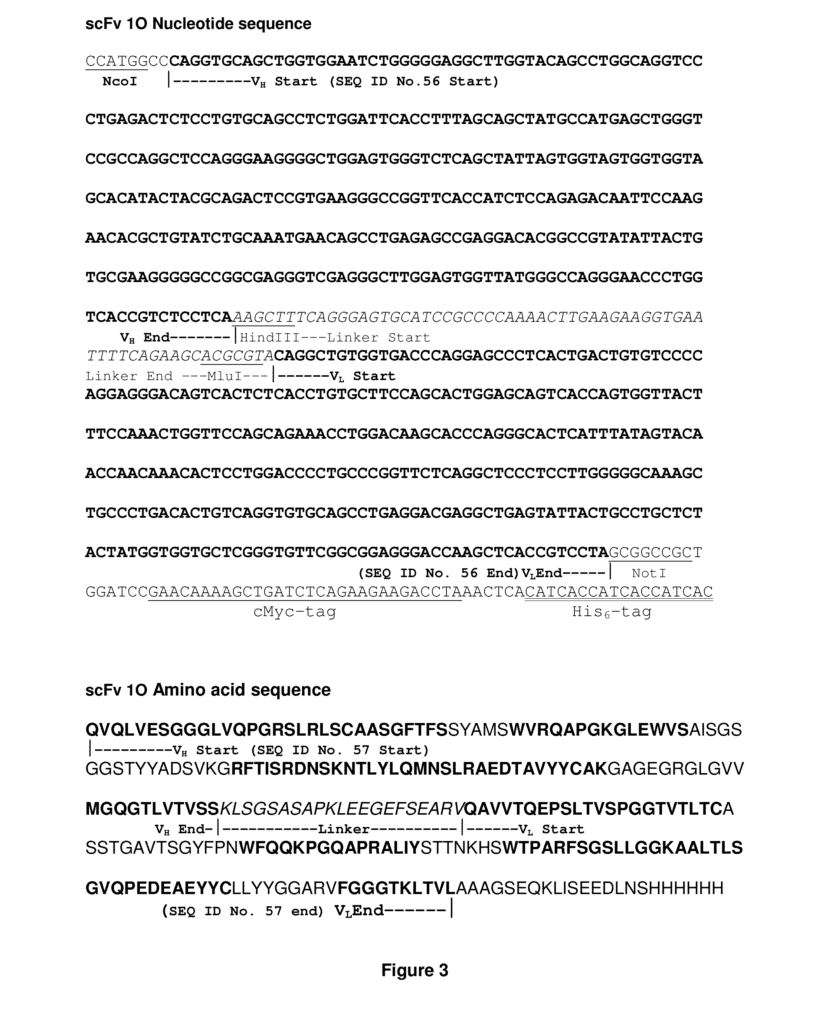
The present invention provides antibodies that bind to the extracellular domains of the human CC chemokine chemokine receptor 4 and are capable of blocking the binding of thymus- and activation-regulated chemokine to CCR4. The invention also includes immunoconjugates, compositions containing such antibodies, and methods and applications involving these antibodies.
Background for Antibodies
G-protein-coupled (GPCR) receptors are the largest family cell surface molecules that transmit signals. They account for more than 2% of all genes in the human genome. The GPCR superfamily shares a membrane topology that includes an extracellular N terminus, an internal C terminus, and seven transmembrane helices (TM). These helices are linked by three intracellular and three extracellular loops. GPCRs can also be referred to by their common topological structure as seven-transmembrane (7TM). These receptors regulate key physiological functions including neurotransmission and hormone and enzyme releases from exocrine and endocrine glands. They also control immune responses, contractions of smooth and cardiac muscles, and blood pressure regulation. The dysfunction of these receptors contributes to many common human diseases. GPCRs play a critical role in cancer progression, according to new experimental and clinical evidence. There is a possibility that certain GPCRs could be good targets for anticancer drugs.
These small, secreted molecules are a growing superfamily of 8-14 kDa proteins characterised by a conserved four cysteine motif. These small molecules, which are secreted by the body, belong to a superfamily of proteins ranging from 8-14 kDa that is characterized by a four-cysteine motif.
Studies have shown that the action of chemokines is mediated by subfamilies G protein-coupled chemokine receptors. One of these receptors is designated chemokine C-C motif receptor 4, or CC chemokine receptor 4 (CCR4). CCR4 ligands include thymus- and activation-regulated-chemokine TARC (also called CCL17) as well as macrophage derived chemokine MDC (also called CCL22). CCR4 can also bind to RANTES and MCP-1, and signaling in response to those ligands have been reported.
CCR4 may be involved in the chemotaxis of T cells and the migration to inflammation sites of phagocytic cell. CCR4 expression is preferentially found on regulatory T (Treg), and T-helper cells type 2 (Th2), while other healthy tissues or cells only show a limited amount of expression.
Tumour Cells, especially adult T-cell leukaemia/lymphoma cell, may be positive CCR4″ Skin involvement is related to expression of CCR4 in tumour cells. Typically, certain T-cell cancers are found on the skin. CCR4 can be found in high concentrations, for example, in lesions of cutaneous T-cell lymphoma. CCR4 expression has been detected in certain solid tumours as recently as WO2009/037454. CCR4 is thought to be a precursor in the carcinogenesis process of solid tumours. This includes cancers of the cervix and oesophagus as well as those of the brain, ovary or prostate. Both haematological as well as non-haematological tumour cells can express CCR4. These cancers can be diagnosed, monitored, and treated with anti-CCR4 antibody.
CCR4 plays an important role both in normal immunity and tumour immunity. CCR4 is expressed by a significant proportion of CD4+CD25+ T-cells that are regulatory (Tregs). (Baatar and colleagues, 2007b). These Tregs suppress the immune response through various mechanisms. It has also been shown that these Tregs can inhibit tumour-specific immunology. The number of Tregs that infiltrate the stroma or the tumour, as well as the lymph nodes draining the tumour, is correlated with a worse outcome for a variety cancers. In studies on mouse models, reducing Tregs activity led to an increase in endogenous immunity against tumours and the efficacy anti-tumour innovations by the immune system. Inhibiting Treg function in tumour immunotherapy is therefore a promising strategy. The inhibition of Tregs can be achieved in several ways: by killing them (depletion), interfering their suppressor function, changing their trafficking patterns or changing their differentiation.
In a subset CCR4+ lymphoma/leukaemia patients, tumour cells function as Tregs, contributing to tumour survival against host antitumour immunity responses. MDC and TARC, produced by cancer cells and tumour microenvironment, attract CCR4+Treg cells to tumours. They create an environment that allows tumours to escape host immune responses. Patients with the following cancers have a higher frequency of Tregs: Breast cancers, Colorectal Cancers, Oesophageal Cancers, Gastric Cancers, Hepatocellular Carcinomas, Lungs cancers, Melanomas, Ovarian and Pancreatic cancers. It has been shown that Treg cells create an environment that is favorable for tumours. Blocking the interaction between CCR4 ligands like MDC and CCR4 could therefore be helpful in the prevention or treatment of cancers. This is especially true for the cancers mentioned above. In a SCID model of mice, it was reported that antibody to human MDC/CCL22 could block the infiltration into human ovarian tumors. The Treg cells in solid tumours of humans are believed to prevent immune response development, which may contribute to slowing tumour growth and metastasis. The killing of Tregs in tumour masses, or the prevention of Treg migration to tumour sites, by using a monoclonal MAb directed against CCR4 could result in an enhanced immune response towards solid tumours and act as a complement to conventional cytotoxic and anti-hormonal treatments.
Cancer is responsible for 13% of human deaths. According to the American Cancer Society 7.6 million people worldwide died of cancer in 2007. There is a need for more anti-cancer therapies.
CCR4 is known to be involved in immune disorders and inflammation. Th2 cells, basophils and mast cells are important cells for the allergic response of the skin and lung. In bronchial biopsy samples of allergen-challenged asthmatics, there are several reports that describe the presence CCR4-expressing cells, and their concomitant CCR4 ligands, MDC and TARC. (Panina Bordignon et. al., 2001). CCR4+T cells are found in greater numbers in patients suffering from atopic skin disease. The number of CCR4+T cells decreases when the condition improves. The humanized SCID mice model of asthma was used to show that blocking CCR4 by antibodies before allergen challenge decreased allergic airway inflammation as well as levels of Th2cytokines. Asthma patients may benefit from the lung delivery of blocking antibodies to reduce CCR4+T cells. A CCR4 blocking anti-body delivered to the skin could be a promising treatment for atopic dermitis.
In allergic asthma the presence of high allergen-specific IgE levels is a reflection on an aberrant T2 cell immune reaction to commonly inhaled environment allergens. Asthma can be characterized by an infiltration of Th2 cells and eosinophils, and the production of Th2 chemicals. Dendritic (DC) cells continuously sample foreign antigens and present them to T-cells. Upon activation by DCs allergen-specific cytokines such as IL-4, IL-5, and IL-13 are produced in the diseased airways. These cytokines control extravasation of leukocytes, goblet-cell hyperplasia, and bronchial Hyper-Reactivity (BHR). TARC and MDC, produced by DCs, induce the migration of Th2 but not Th1 cell through activating CCR4(Perros et.al. 2009). In murine asthma models, treatment with anti TARC antibodies decreased the number of CD4+ T-cells and eosinophils, as well as the production of Th2cytokines, and the hyperresponsiveness of the airways after allergen stimulation (Kawasaki and al, 2001). CCR4-deficient mouse models showed no protection from airway inflammation or BHR (Chvatchko and al., 2000). Perros et. al., 2009) showed that blocking CCR4 using antibodies before allergen challenge decreased allergic airway inflammation and the levels of Th2 in the lungs. These results indicate that CCR4 blocking is a viable strategy to inhibit allergic inflammation in people.
Treg cell suppression of dendritic (DC) cells can facilitate the progression and development of disease, especially infectious diseases and cancer. Anti-CCR4 antibody that can block Treg cell suppression of dendritics cells could be used as adjuvants for vaccines. Anti-CCR4 antibodies may therefore enhance the therapeutic effects of vaccines, enhancing in particular the vaccine-induced immunity response.
2007). “CCR4-binding compounds were reported to be effective in the treatment of murine allergic inflammation” (Purandare, Burdi and Burdi, 2007. 2007). A CCR4-binding drug was reported to have a reasonable potency in the presence of TARC, since CCR4 dependent leucocyte recruitment to the peritoneum was reduced by 90%. Yokoyama, along with colleagues, presented a quinazoline-targeting derivative that was effective in reducing hypersensitivity in a mouse (Yokoyama et. al., 2008b). A derivative of this compound also proved effective in a similar mouse in vivo model after oral administration (Yokoyama et. al., 2009). A group of scientists identified CCR4 antagonists recently using an in silico modeling approach (Bayry, et. al., 2008; Davies, et. al., 2009). The authors discovered molecules that bind to the transmembrane area by docking compounds with a model of CCR4. Sixteen compounds inhibited CCR4 mediated migration of CCRF CEM cells. CCR4 antagonists have been tested in vivo for their adjuvant functions with Mycobacterium tbsis and hepatitis B vaccinations. Both cellular and humoral immunity was enhanced. The observed effect has been attributed to the inhibition of Treg (Bayry, et. al., 2008; Davies, et. al., 2009). It is well-known that Treg cells have a high CCR4 expression (Baatar, et al. 2007b). It is thought that the observed effect can be used not only for vaccinations against infectious diseases, such as those caused by viruses, bacteria, mycobacteria, or parasites like protozoa, but also cancer vaccines.
The pharmacological advantage of antibodies over small molecules drugs is well-known in the field. To our knowledge, the only antibody that is currently being developed against CCR4 is KW-0761 from Kyowa Hakko. This antibody, however, is only effective by ADCC and does not block ligand-mediated signals through CCR4 receptor. The antibodies described in the invention should be superior to other antibodies in modulating immune responses via Tregs.
Cancer treatment is another application of modulating Tregs. Tregs inhibit tumour-specific immune responses and their increased number correlates with poor prognosis in certain cancers. In mouse models, reducing Tregs activity increases endogenous antitumour immunity and the effectiveness of active immune interventions. Inhibiting Treg function in cancer immunotherapy is therefore a worthwhile strategy (Curiel 2008; Ruter and al. 2009). This inhibition can be achieved by either modulating Tregs or directly killing them.
Other molecules on Tregs which are targeted for cancer treatment or improved cancer vaccine effects include GITR (glucocorticoid-induced tumour necrosis factor receptor-related gene) (Levings et al, 2002), Toll-like receptors (TLR) are expressed ubiquitously on a variety of mammalian cells, including human Tregs (Yang et al, 2004, Rutter et al, 2009) and Cytotoxic T lymphocyte antigen-4 (CTLA-4; CD152) (Sutmuller et al. 2001). Two human monoclonal antibodies are under investigation-ipilimumab (MDX-010; Bristol-Myers Squibb/Medarex) and tremelimumab (CP-675,206; Pfizer). Two human monoclonal antibodies are under investigation-ipilimumab (MDX-010; Bristol-Myers Squibb/Medarex) and tremelimumab (CP-675,206; Pfizer).
GPCRs have complex structures and are therefore considered “difficult targets” for raising specific antibodies. Raising specific antibodies is difficult because of their complex structures. The membrane fractions of lysed cell membranes cannot be readily purified, nor can they be produced recombinantly in different expression systems to produce correctly folded soluble protein. “To the inventors’ best knowledge, all previous attempts to produce anti-GPCR antibody using phage displays have failed.
Hoogenboom and colleagues (1999) describe the difficulties in generating antibodies to GPCRs. Furthermore, Sui et al. (2003) describe the difficulties in obtaining human antibodies against GPCR chemokine CXCR4 receptors and report that despite using the step-back selection method with the pathfinder technique, no specific antibodies were identified. In the field of GPCRs the generation of specific antibody remains a challenge.
BD Pharmingen sells a murine monoclonal antigen called 1G1 that reacts with the human CCR4. This antibody can be used to stain immunofluorescently, but it is not neutralising.
Ishida et. al. (2006) disclose KM2760, a chimeric CCR4 antibody. The authors report that the antibody does not inhibit CCR4 binding to its ligands MDC and TARC.
Click here to view the patent on Google Patents.
Leave a Reply