Invented by John R. Desjarlais, Seung Y. Chu, Holly M. Horton, Matthew J. Bernett, Xencor Inc
The market for compositions for the treatment of IgE-mediated diseases is driven by several factors. Firstly, the prevalence of these conditions is increasing globally. According to the World Allergy Organization, allergic diseases affect up to 30% of the world’s population. This has led to a growing demand for effective treatments for these conditions. Secondly, there is a significant unmet need for safe and effective treatments for IgE-mediated diseases. Current treatments such as antihistamines and corticosteroids are often associated with side effects and may not be effective for all patients. This has created an opportunity for new compositions that can provide better outcomes for patients.
There are several types of compositions that are being developed for the treatment of IgE-mediated diseases. One of the most promising is monoclonal antibodies. These are laboratory-made antibodies that can target specific proteins in the immune system that are involved in the development of IgE-mediated diseases. Monoclonal antibodies have shown great promise in clinical trials and have been approved for the treatment of conditions such as asthma and atopic dermatitis.
Another type of composition that is being developed is allergen-specific immunotherapy. This involves exposing patients to small amounts of the allergen that triggers their IgE-mediated disease. Over time, the immune system becomes desensitized to the allergen, reducing the severity of the patient’s symptoms. Allergen-specific immunotherapy has been shown to be effective for the treatment of allergic rhinitis and asthma.
There are also several other compositions that are being developed for the treatment of IgE-mediated diseases. These include small molecule inhibitors, gene therapies, and cell-based therapies. While these compositions are still in the early stages of development, they show great promise for the future treatment of these conditions.
In conclusion, the market for compositions for the treatment of IgE-mediated diseases is growing rapidly. This is driven by the increasing prevalence of these conditions and the significant unmet need for safe and effective treatments. Monoclonal antibodies and allergen-specific immunotherapy are currently the most promising compositions for the treatment of these conditions. However, there are several other compositions that are being developed that show great promise for the future. As research in this area continues, we can expect to see significant advances in the treatment of IgE-mediated diseases in the coming years.
The Xencor Inc invention works as follows
The present invention relates primarily to immunoglobulins which bind IgE with high affinity and FcRIIb, and are capable of inhibiting membrane-anchored IgE expressing cells. These compositions can be used to treat IgE-mediated diseases, such as allergies and asthma.
Background for Compositions for the treatment of IgE-mediated diseases
Allergy diseases and conditions such as asthma and allergic rhinitis have increased in prevalence over the last few decades. They now affect between 10-40% the population of industrialized nations. Allergic diseases can have a profound impact on the quality of your life and even result in death in severe cases. Allergies affect millions of people and cause the most time missed from school and work. They also have a huge impact on the economy and medical system. As an example, allergy rhinitis, or hay fever, affects at least 22% of the US population, while allergic asthma affects at least 20 millions. In the United States alone, the economic impact of allergy diseases, including the costs associated with health care and lost productivity, was estimated at $6.4 billion during the early 1990s.
Most allergic diseases are caused due to hypersensitivity reactions mediated by immunoglobulin E. IgE is an antibody class that’s normally found in serum at very low concentrations. It is produced when IgE-secreting cells express the antibody at their surface. Allergy patients produce high levels of IgE that bind to normally harmless antigens. These IgE molecules circulate through the blood, and bind with IgE-specific IgE receptors found on the surface mast cells and basophils along the mucosal linings of the skin and in circulation. The binding of allergens or antigens to IgE on basophils and mast cells aggregates the receptors and crosslinks the IgE molecules. This triggers the release of neuronal and vasoactive stimulatory mediators like histamines and leukotrienes. Immediate or antibody-mediated reactions are caused by the rapid immune response to antigens by antibody immune complexes, as opposed to delayed or T-cell-mediated reactions. IgE-mediated immunoreactions are specifically called type I hypersensitivity reaction.
The high affinity IgE receptor (Fc?RI), is the key mediator of immediate allergic manifestations. Fc?RI can be found on other cell types, including platelets, eosinophils and antigen-presenting monocytes or dendritics cells, in addition to mast and basophils. Fc?RII is another receptor for IgE. It’s also called CD23 or low-affinity IgE Fc. Fc?RII can be found on a wide range of cell types, including B lymphocytes and platelets. It is also expressed by macrophages. Fc-RII could play a part in the feedback regulation IgE expression, and then Fc-RII surface expression.
Since IgE is a key mediator of most allergic reactions it has been of interest to develop treatments that control IgE in the body, and regulate IgE syntheses. There are several strategies that have been proposed for treating IgE-mediated allergies by lowering IgE levels. One method involves binding the? chain of IgE to the Fc receptor binding site. Omalizumab, a recombinant monoclonal anti IgE antibody which binds IgE at the same Fc as Fc?RI is an example. Omalizumab reduces the total serum or circulating IgE levels in atopic individuals, which in turn decreases the amount of antigen specific IgE that can attach to tissue mast cells and Basophils and cause sensitization. The symptoms of allergic disease will also decrease. It is interesting to note that serum IgE increases after the start of treatment due to the formation of an omalizumab/IgE complex. These levels can remain high for up to one year after therapy has been stopped. This issue can lead to false negatives in diagnostic tests, so IgE levels should be checked regularly. In order to reduce IgE, it is necessary to improve methods and compositions. IgE?mediated diseases and symptoms.
The present disclosure provides novel molecules of coengagement that bind IgE with Fc?RIIb at high affinity. It also includes compositions containing such molecules and methods for using these novel molecules to treat IgE mediated disorders. The invention’s coengagement molecules are capable of inhibiting membrane IgE-expressing cells and FcRIIb-expressing cells. IgE+Fc?RIIb+ cells. The invention’s coengagement molecules are also capable of binding IgE circulating in the blood. “The inhibitory methods described herein involve contacting IgE+FcRIIb+cells with a coengagement molecules that coengages IgE on the surface of the cell.
The compositions disclosed include coengagement molecules that are capable of coengagement IgE with Fc?RIIb on the surface of the cell. In one embodiment, the coengagement molecule comprises an immunoglobulin capable of binding IgE with high affinity and FcRIIb. The coengagement molecules in the invention coengage membrane-anchored IgE on a cell surface with FcRIIb and bind FcRIIb preferably at a Kd less than 100 nM. In one preferred embodiment, the coengagement molecule comprises an immunoglobulin. In another preferred embodiment, said immunoglobulin comprises an antibody, whose Fv region specifically binds IgE. In a preferred embodiment of the invention, said antibody binds circulating IgE and membrane-anchored IgE. In alternative embodiments, the antibody binds only membrane-anchored IgE compared to circulating IgE. In another embodiment, coengagement molecule has a bispecific antigen having a first and second target specific regions, wherein first target specific area binds IgE, and second target specific area binds FcRIIb, with a Kd less than 100 nM. In a preferred form, the first and second targets specific regions are Fv, where the first Fv binds IgE and the second Fv binds Fc-RIIb, with a Kd less than 100 nM. In another embodiment of coengagement molecule, the Fc fusion comprises an Fc area, which binds Fc-RIIb at a Kd less than 100 nM. The Fc fusion of the immunoglobulin is bound to IgE in this embodiment.
In one embodiment, coengagement molecule binds to Fc?RIIb. The affinity of the binding has a Kd lower than about 100nM. For example, it is less or equal than 95nM or 90nM. It can also be less or equal than 85nM or 80nM.
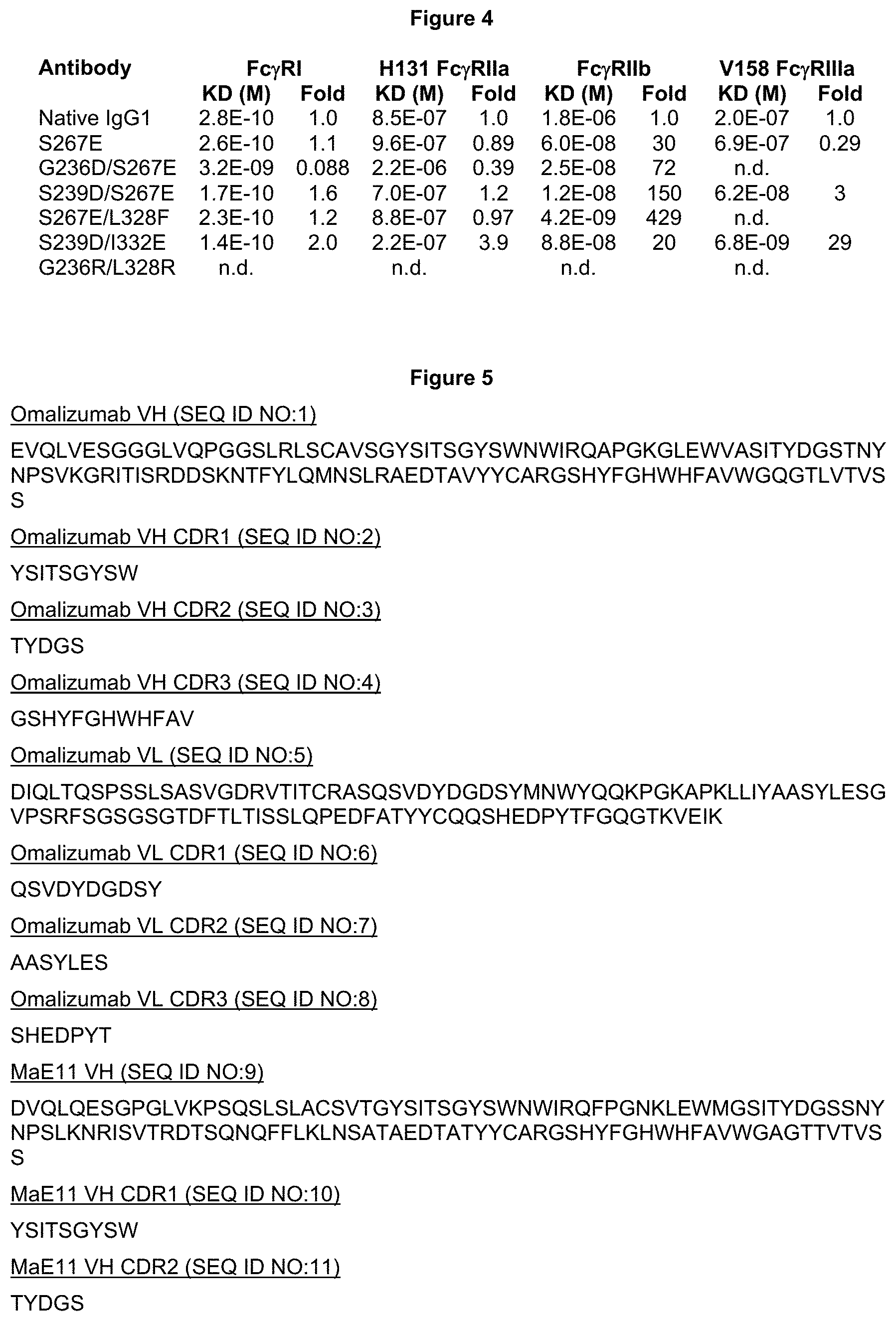
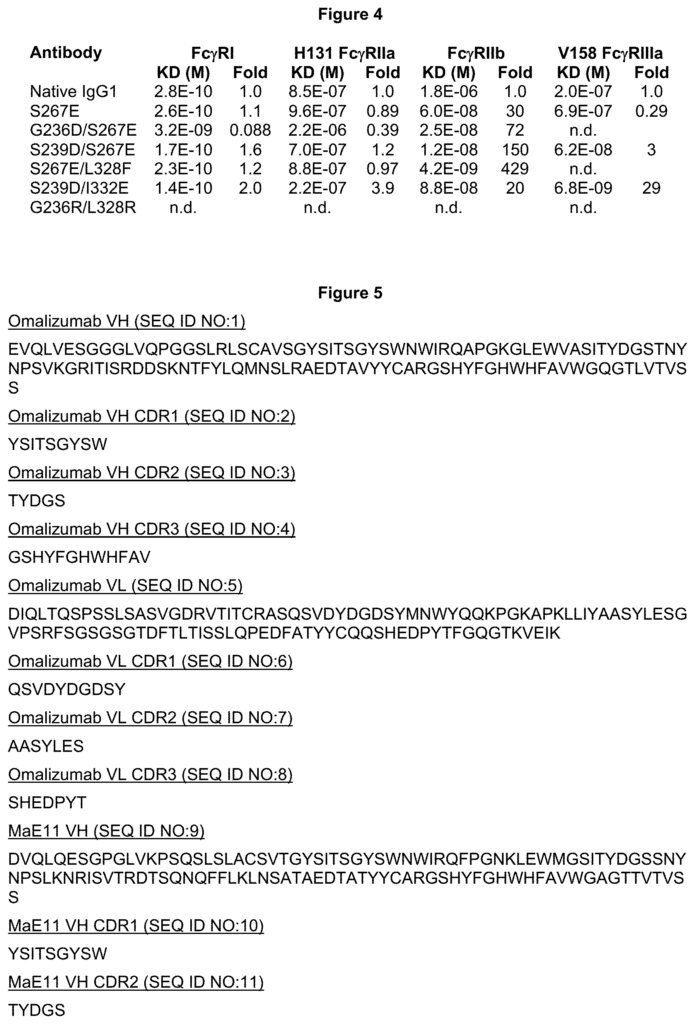
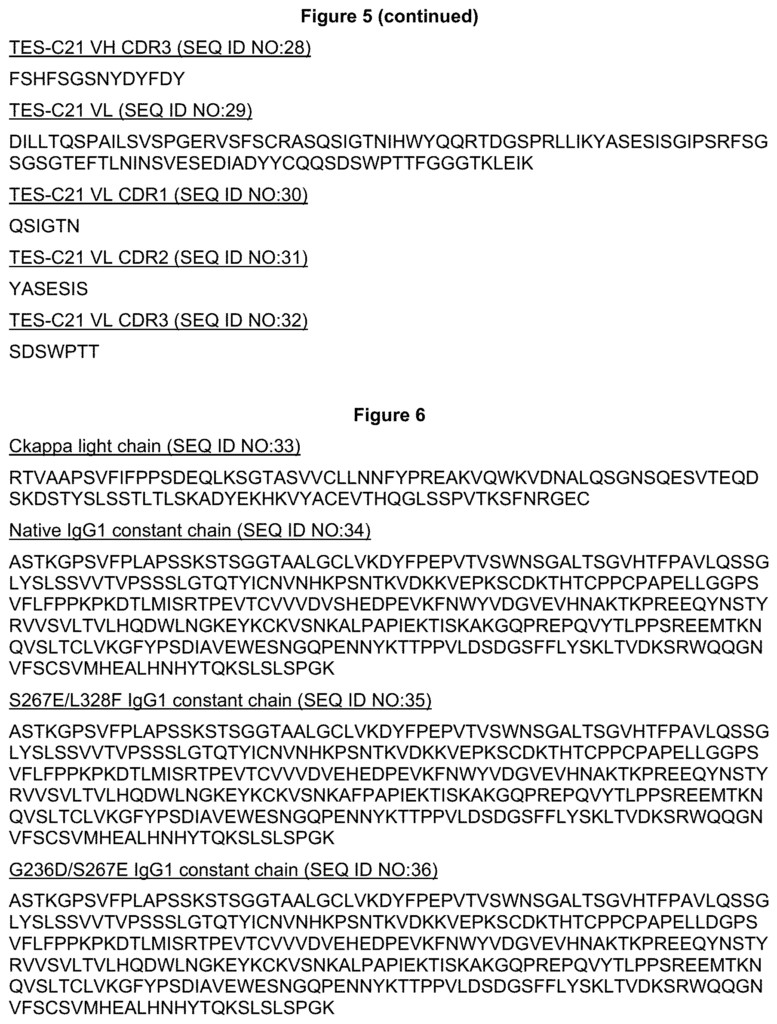
In one embodiment, a variant of the parent immunoglobulin is used in a coengagement molecule. In one embodiment, the variation immunoglobulin includes a variant Fc-region, which comprises one or two (e.g.) modifications compared to a parental Fc-region, and wherein the modification(s), are located at positions chosen from the group consisting 234, 235, 236, 236, 237, 239, 265, 266, 267, 268, 298, 325, 326, 327, 328, 330, 331, 332, 3322, 3322, 3322, 3322, 3322, 3322, 3322, 3322, 329, 328, 328, 328, 328, 328, 328, 328, 328, 328, In another embodiment, the modification(s), according to the EU Index, are located at positions chosen from the group consisting 234, 235 236, 237 266, 267 268, 327 and 328. In another embodiment modification(s), according to the EU Index, are located at positions chosen from the group consisting 235, 236 266, 267 and 328. In another embodiment modification(s), are at positions chosen from the group consisting 235, 239, 266 267, 268 and 328 according to the EU Index. In another embodiment, the modification(s) is at positions that are selected from the group consisting 234, 236, 236, 236, 239, 266, 268, 267, 268 and 328 according to the EU Index.
In The In The In The In Select In Select In The
In one embodiment, the modification(s), if any, results in at least one combination of substitutions, namely: 235Y/267E; 236D/267E; 239D/268D; 239D/267E; 239D/332E; 267E/268D and 267E/268E. The numbering of these parts is according to a EU index.
In one embodiment, modifications disclosed herein reduce affinity for at least one receptor relative the parent immunoglobulin. Said receptor is selected from a group consisting FcRI, FcRIIa and FcRIIIa. In this embodiment the immunoglobulin variations disclosed herein can mediate a reduced ADCC or ADCP compared to the parent antibody. In an alternative embodiment, the modifications revealed herein increase affinity for at least one receptor relative the parent immunoglobulin. Said receptor is selected from a group consisting FcRI, FcRIIa, or FcRIIIa. This embodiment may allow for increased ADCC and ADCP relative the parent immunoglobulin.
The invention also discloses methods for engineering novel coengagement molecules including immunoglobulin compounds.
Also described herein are nucleic acid isolates encoding coengagement molecules including immunoglobulins.” Vectors containing the nucleic acid, which can be operably linked with control sequences, are also disclosed. Host cells containing vectors are also disclosed, as well as methods for producing coengagement molecules and recovering them if desired.
Also, disclosed herein are the coengagement molecules which comprise the immunoglobulins revealed herein. Coengagement molecules can be used in therapeutic products. The coengagement molecules may, in one embodiment be antibodies.
Also, compositions are disclosed that include coengagement molecules as described herein and a physiologically- or pharmaceutically-acceptable carrier or diluent.
Also disclosed are methods for inhibiting IgE+FcRIIb+cells. The described methods for inhibiting cells involve contacting an IgE+FcRIIb+ with a coengagement-molecule that binds to FcRIIb at a Kd less than 100 nM. In the most preferred embodiments of this invention, said coengagement molecules coengage IgE with Fc?RIIb at the surface of the cell. In preferred embodiments the inhibition methods include contacting an IgE+FcRIIb+cell with an antibody. The antibody has an Fc-region that binds FcRIIb at a Kd less than 100 nM. In other embodiments the Fc region binds native IgG1 with a greater affinity than Fc?RIIa or Fc-RIIIa. In alternative embodiments, contacting IgE+Fc-RIIb+cells with a coengagement is comprised of a bispecific antigen comprising a Fv and Fv regions, where the first Fv binds IgE and the second Fv binds Fc-RIIb at a Kd less than 100 nM. In alternative embodiments, methods include contacting IgE+FcRIIb+cells with a coengagement molecular, wherein the coengagement molecular is an Fc-fusion containing an Fc area, wherein this Fc region binds FcRIIb at a Kd less than 100 nM.
The method includes contacting an IgE+Fc?RIIb+ cell with a coengagement molecule, wherein said coengagement molecule binds IgE and Fc?RIIb with a Kd of less than about 100 nM. The method involves contacting a cell that is IgE+FcRIIb+ with a coengagement-molecule. This coengagement-molecule has a binding affinity for IgE and the FcRIIb molecule of less than 100 nM.
This method includes contacting an IgE+Fc?RIIb+ cell with a coengagement molecule, wherein said coengagement molecule binds IgE and Fc?RIIb with a Kd of less than about 100 nM. This method involves contacting an IgE+FcRIIb+cell with a coengagement-molecule, in which said coengagement-molecule binds IgE with a Kd less than 100 nM.
The coengagement molecules are also described in terms of their therapeutic and diagnostic applications. In one embodiment, coengagement molecules are used in treating IgE-mediated disorders. In a preferred embodiment, the coengagement molecules disclosed herein are used to treat one or more IgE?mediated disorders, such as autoimmune diseases, inflammation diseases, etc. Immunoglobulin IgE-mediated disorders. The compositions disclosed herein may treat allergic and/or atopic disorders, including but not limited to allergies, allergic rhinitis or conjunctivitis/rhinoconjunctivitis. The present invention comprises a treatment method that involves administering to a patient a therapeutic dose of a coengagement molecules that coengages IgE with Fc?RIIb at a cell surface.
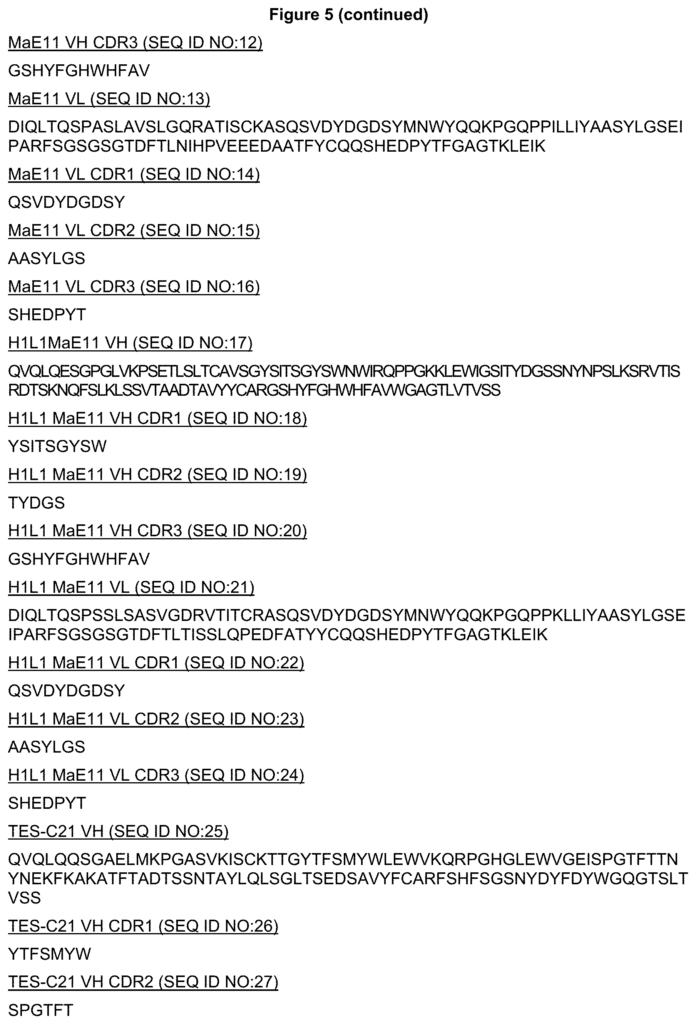
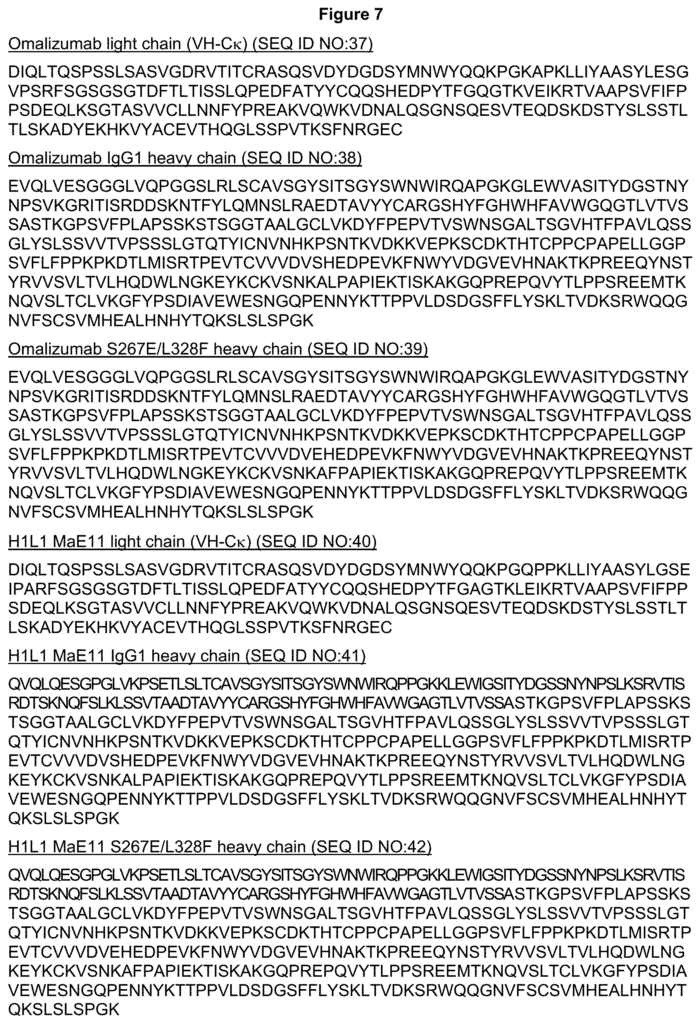
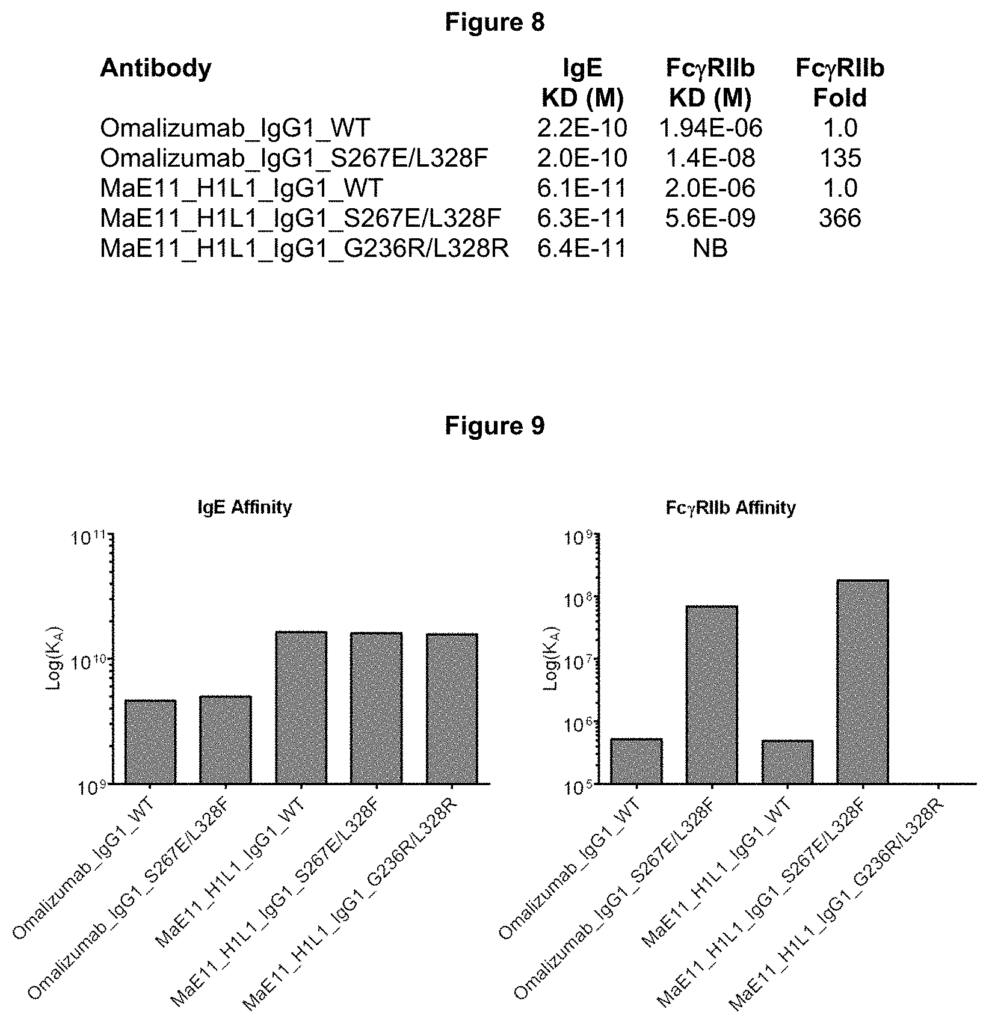
The coengagement molecules described herein mimic the inhibitory effect of coengagement between membrane-anchored IgE and Fc?RIIb in B cells. As an example, herein described are variant anti IgE antibodies engineered so that the Fc-domain binds Fc-RIIb up to a?430-fold higher affinity. The Fc?RIIb-binding-enhanced variants (IIbE), compared to native IgG1, strongly inhibit BCR induced calcium mobilization in primary human IgE+ B cell. A novel treatment for IgE-mediated disease may be the use of a single antibody that inhibits B cell functions through coengagement of cognate IgE Fc?RIIb and BCR. IgE-mediated disorders include asthma and allergic reactions.
The disclosure provides that “coengagement molecules” can be configured in a number of ways, as described below. In one embodiment, the coengagement molecule comprises an immunoglobulin which binds IgE with high affinity and FcRIIb. This embodiment binds Fc?RIIb and membrane-anchored IgE on the surface of a cell with a Kd less than 100 nM. In another embodiment the coengagement molecule has a bispecific region with two target specific regions, with the first region binding IgE, and the second region binding FcRIIb. The Kd is less than approximately 100 nM in this embodiment. However, in other embodiments, it can bind FcRIIb at a lower Kd than 10 nM. In a preferred embodiment, the coengagement molecule comprises a bispecific antigen, the first and second targets specific regions being Fv regions. The first Fv area binds IgE and the second Fv area binds Fc-RIIb, with a lower Kd than 100 nM. In a second embodiment, the coengagement molecule comprises an Fc fusion containing an Fc-region, which binds Fc-RIIb at a Kd less than 100 nM. The Fc fusion of the immunoglobulin is bound to IgE in this embodiment.
Click here to view the patent on Google Patents.
Leave a Reply